Certificate of prescribed authority for the purposes of section 80DDB 1.
Name of the Patient
2.
Address
3.
Father’s name
4.
Name and address of the person on whom the patient is dependent and his relationship with the patient.
5.
Name of the disease or ailment (please see rule 11DD)
6.
For diseases or ailments mentioned in item (i) of clause (a) of sub-rule (1), whether the disability is 40% or more (Please specify the extent).
7.
Name, address, registration number and qualification of the specialist issuing the certificate, along with the name and address of the Government hospital [see rule 11DD(2)] Verification This is to verify that I, Dr.____________________________________________________ s/o (w/o) Shri_____________________, in the case of the patient Shri/Smt./Ms.________________________, after considering the entire history of illness, careful examination and appropriate investigations, am of the opinion that the patient is suffering from______________________________disease/ailment during the previous year ending on 31st March,_______________________ I also certify (only in case of neurological disease) that the extent of disability is more than 40%) (Strike off, if not applicable). I certify that the information furnished above is true to the best of my knowledge. Date Place
_______________ _______________
Signature (Name and Address)
To be countersigned by the Head of the Government hospital, where the prescribed authority is a specialist with post-graduate degree in General or Internal Medicine. Date Place
after considering the entire history of illness, careful examination and appropriate investigations, am of the opinion that the patient is suffering from______________________________disease/ailment during the previous year ending on 31st March, ...
Page 1 of 1. NEW YORK STATE PUBLIC HIGH SCHOOL ATHLETIC ASSOCIATION. WRESTLING MINIMUM WEIGHT ASSESSMENT. PARENTAL AWARENESS FORM. The appropriate and healthful control of body weight for wrestlers has been a concern of athletes, coaches,. athletic t
Policy No/Certif No. Policy Holder`s Name. Address. Telephone No. Email ID ... for our record, Your banker should be a participant of NEFT/RTGS Facility.
Performs custodial cleaning and light maintenance of school site classroom, multi-use, office, immediate grounds, and related facilities. Custodian I. Notices may ... available at the Human Resources Office and return before: Current Employees: If yo
Degree applied for⦠... B: (To be completed by the Referee). 5. How long and in what capacity, have you known the candidate? ... Post Graduate Admissions,.
O. Publishing House â weekly (1 to 2 hours). O. Office Phone â weekly (1 hour). O. Special Events (e.g., Walkathon, Multicultural Dinner, etc.) I have the following ...
Hosted Reception 6pm; Call to Dinner 7pm ... Authorized by the DCCWC, Lanny Hickman, Treasurer, All funds solicited in connection with this event are by the.
LIC Policy Maturity Discharge Form (English & Hindi version) FORM No 3825.pdf. LIC Policy Maturity Discharge Form (English & Hindi version) FORM No 3825.
Rev 11/11. DOCTORAL ORAL EXAMINATION FORM. This form must be completed and sent to the Doctoral Candidacy Advisor,. 450 DuBourg Hall, AT LEAST TWO WEEKS PRIOR TO THE EXAMINATION. STUDENT'S NAME: ...
Post/zip code: Country: This is the address that your certificate will be sent to. If you want your centre to send it to a different address,. please contact the centre directly. Passport or national ID number: (this must be the ID you will bring wit
thorization at any time and Kiwanis will have thirty (30) days to remove my picture, image, name or other reference to me and/or my business. I hereby release ...
Aug 1, 2015 - The Park , 17, Park Street, Kolkata â 700 016. Name. : Address ... For Rs. 1300/- (Rupee one thousand three hundred only) Spot Registration.
Private Health Service Plan Enrollment Form ... Incorporated Business? ... Administration Inc. (The Heritage) establishes and manages a Private Health Services ...
Installs, configures, troubleshoots, and services networked computer workstations and related equipment and software used in administrative and instructional lab environments. Designs, installs, configures, monitors, operates, and maintains server ha
Have you ever tried cigarettes, chewing tobacco, snuff, or dip? ⢠During the past 30 days, did you use chewing tobacco, snuff, or dip? ⢠Do you drink alcohol or use any other drugs? ⢠Have you ever taken anabolic steroids or used any other perf
Whoops! There was a problem loading more pages. Retrying... Whoops! There was a problem previewing this document. Retrying... Download. Connect more apps... Try one of the apps below to open or edit this item. Form BAAk.pdf. Form BAAk.pdf. Open. Extr
Jan 24, 2017 - If you are interested in participating in this examination, please apply on EdJoin.org by : Position May be filled by a Lateral Transfer or from the current eligibility list: Current Employees: please complete an interest form @ delnor
U DVDs of the concert are available for $15 each and may be picked up at. Willamette Valley Music Company, 484 State St., Salem beginning Dec 19 or at re- hearsals starting January 13. Please fill in the information below or fill out a form under. An
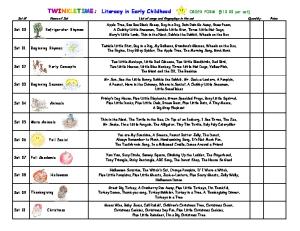
Jack-o-Lantern, A Pum pkin,. A Peanut, H ere is the Chim ney, W here is ... Cloud,. M aking a Snow m an, A W inter D ay, Five H appy Snow m en, T he M itten Song. Set 13. S pring. Earthw orm , Little Sunflow er, G row ing in the Sun, Pussyw illow , D