Focal Atrophy and Cerebrovascular Disease Increase Dementia Risk among Cognitively Normal Older Adults
Caterina Rosano, MD, MPH Howard J. Aizenstein, MD, PhD Minjie Wu, MS Anne B. Newman, MD, MPH James T. Becker, PhD Oscar L. Lopez, MD Lewis H. Kuller, MD, PhD
ABSTRACT Background and Purpose. This study investigated the association of medial temporal lobe (MTL) atrophy and cerebrovascular disease (white matter hyperintensities [WMH], subclinical infarcts) with the risk of developing Alzheimer’s disease (AD) among cognitively normal older adults. Methods. Risk of developing AD was examined for 155 cognitively normal older adults (77.4 years, 60% women, 81% white). The MTL volumes and the presence of WMH and of subclinical infarcts were determined from brain magnetic resonance imaging (MRI) at the beginning of the study. Follow-up cognitive evaluations (average 4.3 years) identified those who developed AD. Results. The presence of either MTL atrophy or subclinical infarcts was independently and significantly associated with a greater risk to develop AD (OR [95% CI]: 4.4 [1.5, 12.3] and 2.7 [1.0, 7.1], respectively). In addition, those participants with both MTL atrophy and at least one brain infarct had a 7-fold increase in the risk of developing AD (OR [95% CI]: 7.0 [1.5, 33.1]), compared to those who had neither of these conditions. Conclusions. In
Received November 17, 2006, and in revised form November 17, 2006. Accepted for publication November 22, 2006. From the School of Public Health, Department of Epidemiology, University of Pittsburgh, Pennysylvania (CR, LHK); Department of Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh, Pennsylvania (HJA, MW); School of Public Health, Department of Epidemiology, and Division of Geriatric Medicine, Department of Medicine, University of Pittsburgh, Pennsylvania (ABN); Departments of Psychiatry, Neurology and Psychology, University of Pittsburgh, Pennsylvania ( JTB); Department of Neurology, University of Pittsburgh, Pennsylvania (OLL, LHK). Address correspondence to Caterina Rosano, MD, MPH, 130 N Bellefield, room 519, Pittsburgh PA, 15213. E-mail:
[email protected].
cognitively normal older adults, markers of neurodegeneration (as reflected by MTL atrophy) and of cerebrovascular disease (as reflected by infarcts on MRI) independently contribute to the risk to develop AD. Key words: White matter, hyperintensity, dementia, focal atrophy. Rosano C, Aizenstein HJ, Wu M, Newman AB, Becker JT, Lopez OL, Kuller LH. Focal atrophy and cerebrovascular disease increase dementia risk among cognitively normal older adults. J Neuroimaging 2007;17:148-155. DOI: 10.1111/j.1552-6569.2007.00093.x
Introduction Reliable clinical indicators of risk of Alzheimer’s disease (AD) do not yet exist, although a number of risk factors have been documented such as the presence of the APOe4 allele, cardiovascular risk factors and lower educational attainment.1 Neuroimaging can increase the accuracy of diagnosis of dementia, and the relatively distinct neurodegenerative topography of AD makes the medial temporal lobe (MTL) and its subregions appropriate ADspecific neuroimaging biomarkers.2-4 Volumetric measures of ventromedial temporal lobe are correlated with memory impairment,5,6 and MTL volumetric changes in cognitively normal older adults are associated with increased risk to convert to clinically ascertained AD.7-10 Furthermore, brain magnetic resonance imaging (MRI) correlates of diffuse subclinical cerebrovascular pathology, such as white matter hyperintensities (WMH) and small brain infarcts, are also associated with worsening of cognitive function over time.11,12 Recently, there has been an interest in examining the relative contribution of focal volumetric changes and diffuse cerebrovascular disease to cognitive
C 2007 by the American Society of Neuroimaging Copyright ◦
148
Table 1.
Neuropsychological and Neurological Tests Used in the Cardiovascular Health Study for Cognitive Assessment
Domain
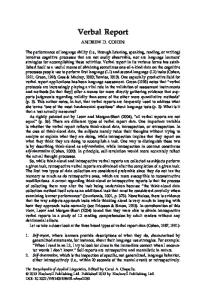
Fig 1. Brain MRI markers. (A) Coronal view of the medial temporal lobe (MTL), obtained from summing hippocampus, parahippocampus, and amygdale. (B) An example of participant with white matter intensities = 4 + (on a 0-9 scale).
impairment.11,13-16,35-39 A few cross-sectional studies have shown that older adults with smaller MTL and greater WMH burden are more likely to have mild cognitive impairment14 or dementia.15,16 However, the question remains as to whether the co-occurrence of focal brain atrophy and of diffuse subclinical cerebrovascular disease in older adults who are cognitively normal is a marker of an increase in the risk to develop AD over time. Understanding the relationship between focal atrophy in areas linked to AD pathology and diffuse cerebrovascular disease may help to understand to what extent intervention on cerebrovascular risk factors may help reduce risk of conversion to AD among cognitively normal older adults, before they experience any sign of cognitive impairment. In this article, we used novel longitudinal data from the Cardiovascular Health Study to examine the relative contribution of MTL atrophy and of burden of diffuse cerebrovascular disease (WMH and infarcts, Fig 1) to define the best predictive model to identify those cognitively normal older adults who will develop AD over time. Materials and Methods Study Population Participants were part of the Cardiovascular Health Study cohort, a longitudinal ongoing study of 5888 adults aged 65+ who were recruited from Medicare Part A lists beginning in 1988-1989 at 4 clinical sites (Forsyth County, NC; Sacramento County, CA; Washington County, MD; and Pittsburgh, PA).17 The present study used data from the Pittsburgh cohort. Brain MRI were originally acquired in Pittsburgh as part of the CHS in 1997-1999 (n = 523). As part of an ongoing NIA-funded research
Test
Neuropsychological Battery Premorbid AMNART IQ Raven’s Memory California Verbal Test REY figure delayed recall Construction REY figure copy Block design Language Naming Word generation (letters) Word generation (categories) Psychomotor speed Trails A Executive Trails B/A Functions Stroop color word Neurological examination Motor and sensory Assessment of cranial nerves, motor function tone, abnormal movements, strength, deep tendon reflexes, release signs, plantar response and clonus, cerebellar testing, primary sensory testing (including graphesthesia and stereognosis), gait, and postural stability Mental status Immediate and delayed recall of 3 words, verbal fluency, similarities, clock drawing test, and the Luria 3-hand test of sequencing
project, these images are being retrieved from the optical disks and are being re-read using the automated labeling pathway (ALP). The order in which the brain MRI are being retrieved from the optical disk is essentially random as it follows the ID number. We used the first 199 brain MRI from cognitively normal participants acquired in 1997-1999 and for whom we had complete follow-up data until 2002-2003. Nonsignificant difference was observed between this sample and the original population of 327 cognitively normal with regard to age, gender, race, education, cardiovascular disease, or visual ratings of brain integrity from the MR scans. We also retrieved brain MRI from 10 other cognitively normal participants, but since these died and were lost to follow-up before information on their cognitive status was collected, these could not be included in the analysis. Ascertainment of Cognitive Function The criteria to adjudicate the cognitive status have been previously published.18-20 The participants received a neuropsychological and a neurological evaluation. (see Table 1). A test’s response was classified as abnormal if
Rosano et al: Predictors of Conversion to AD
149
Table 2.
Characteristics of Study Population at Risk for Incident ADa
Total N Age, mean years (SD)∗ White race, n (%) Female gender, n (%)∗ Years of education, mean (SD) Presence of allele 4 APOe, n (%)† 3MSE, mean (SD) Coronary heart disease, n, (%) Diabetes, n (%) Systolic blood pressure, mean (SD) Stroke, n (%) Total brain, mean (SD), cm3 Right MTL, mean (SD),∗∗ cm3 Left MTL, mean (SD),∗∗ cm3 White matter hyperintensity ≥ grade 4, n (%) Subclinical brain infarcts ≥1, n (%) Subclinical basal ganglia infarcts >1, n (%)
Remained Cognitively Normal
Developed Alzheimer’s Disease
Total
116 76.9 (3.4) 93 (80.2) 64 (55.2) 16.6 (4.1) 23 (19.8) 95.3 (4.4) 20 (17.2) 14 (12.1) 131.2 (19.2) 4 (3.4) 1,375 (134) 12.3 (1.5) 11.8 (1.5) 17 (14.6) 27 (23.3) 17 (14.6)
39 78.2 (3.4) 33 (84.6) 28 (71.8) 15.7 (4.1) 12 (30.8) 93.8 (4.5) 10 (25.6) 6 (15.0) 134.1 (20.9) 1 (2.6) 1,308 (153) 11.2 (1.7) 10.6 (1.5) 8 (20.5) 14 (35.9) 11 (28.2)
155 77.4 (3.4) 127 (81.9) 93 (60.0) 16.4 (4.1) 37 (23.9) 94.9 (4.3) 30 (19.3) 20 (12.8) 131.9 (19.6) 5 (3.2) 1,358 (142) 12.0 (1.6) 11.5 (1.6) 25 (16.1) 41 (26.4) 28 (18.1)
3MSE = Modified Mini Mental State Exam; MTL = medial temporal lobe; SD = standard deviation. a Excludes individuals developing mild cognitive impairment or vascular dementia during follow-up. ∗ P < 0.05; ∗∗ P ≤ 0.0001. † n = 4 missing.
it was >1.5 standard deviation (SD) below individuals of comparable age and educational level. If > 2 tests of the same domain were abnormal, then the domain was considered abnormal. Telephone interviews at 6 months intervals and hospitalization records were collected for all participants from time of the brain MRI through 20022003. For those participants who did not come to the clinic for cognitive evaluation (n = 76, of which n = 24 had died by the end of follow-up), information on cognitive status was collected using the Telephone Interview Cognitive Status (TICS), by interviewing the physician and the proxy using the Informant Questionnaire for Cognitive Decline in the Elderly (IQ CODE). Further information on cognitive and health status from 1989 onward was collected, including changes in modified MiniMental State Exam (3MSE) score.21 The diagnosis of mild cognitive impairment (MCI) was made if cases presented memory deficits, OR deterioration in other cognitive domains (eg, language, executive functions, visuoconstructional abilities), OR had one abnormal test in at least 2 cognitive domains, without sufficiently severe cognitive function impairment, or loss of instrumental activities of daily living to constitute dementia. Onset of MCI status was not ascertained as it was not possible to capture those cases converting to cognitively normal (CN) or to dementia. Dementia was diagnosed if a participant with a history of normal intellectual function before the onset of cognitive
150
Journal of Neuroimaging Vol 17 No 2 April 2007
abnormalities presented with at least 2 of the 6 cognitive domains abnormal, and with severe limitations of activities of daily living. After the clinical evaluation, one of us (O.L.L.) made an initial classification: dementia, MCI, or normal. A committee of neurologists, psychiatrists, and neuropsychologists reviewed the MCI and dementia cases and reached consensus on cognitively normal, MCI, and dementia cases. The adjudication committee had access to the CHS data, the historical CHS cognitive test scores, vision and hearing test results, and the participant’s history of alcohol intake, as well as all relevant CHS data, including medical record reviews. Based on the information available, the adjudication committee classified all CHS participants, including those who were dead by 2002-2003. Dementia type was adjudicated using NINDS-ADRDA and ADDTC criteria.22 By the end of follow-up, of the 199 participants who were cognitively normal at the beginning of the study, 116 (58%) remained cognitively normal by the end of follow-up, 39 (19.6%) converted to AD (35 met criteria for pure AD and 4 met criteria for AD mixed with vascular dementia), 1 converted to vascular dementia, and 43 (22%) developed signs of MCI. The proportion of new AD cases was 4.2%/year, which is consistent with the annual AD incidence rate observed in adults age 75 years and older.23,24 Analyses were repeated before and after exclusion of the 4 participants with mixed AD and also
for those converting to Probable and to Possible AD (n = 21 and n = 14, respectively). Brain MRI
The MR images were collected in 1997-1999 at the University of Pittsburgh Medical Center MR Research Center using a 1.5T Signa scanner (GE Medical Systems, Milwaukee, WI) with high performance gradients (4 G/cm and 150 T/m-s).25 The subjects were positioned in a standard head coil and a brief scout T1-weighted image obtained, followed by standardized sagittal T1-weighted spin-echo images, spin density/T2 weighted and axial T1-weighted images. A volumetric spoiled gradient recalled acquisition (SPGR) sequence with parameters optimized for maximal contrast among gray matter, white matter, and cerebrospinal fluid was acquired in the coronal plane (TE/TR = 5/25, flip angle = 40◦ , NEX = 1, slice thickness = 1.5 mm/ 0 mm interslice). Semiquantitative brain MRI measures included centralized readings performed by radiologists who were blind to the participants clinical characteristics.25 For this study, we used data on the number and locations of infarctions >3 mm, the severity of WMH (Fig 1B), and a measure of head size. Subclinical brain infarcts were defined as masses ≥3 mm that lacked a vascular distribution and were hyperintense on both spindensity and T2-weighted sequences and included both small infarcts (mostly subcortical, lacunar infarcts, with a size ≤ 20 mm) or larger infarcts (either subcortical or cortical, size >20 mm, with a median anteroposterior diameter of 50 mm and a median right-left diameter of 60 mm). Since most of the participants who had large infarcts also had small infarcts, we pooled these two categories into the binary variable “at least one subclinical brain infarct.” Risks associated with the two subgroups of infarcts (small lacunar vs large) were also examined separately. The severity of WMH was assessed on a 10-point scale from 0 to 9, according to an atlas of predefined visual standards.26 WMH ≥ grade 4, and the presence of at least 1 subclinical brain infarct were considered markers of cerebrovascular disease. The degree of ventricular enlargement was assessed on a 10-point scale from 0 to 9, according to an atlas of predefined visual standards.26 The largest right-left diameter from the inner table of the skull measured on any one slice was used as indicator of total cranial volume. ALP Volumetric Measures of Gray Matter
Gray matter voxel counts of the MTL were obtained using the ALP.27,28 ALP uses an automated computational approach and a fully deformable registration algorithm to localize, label, and measure the number of voxels of
gray matter, white matter, and cerebrospinal fluid (CSF) of individual regions in each individual’s MR image. Precision, repeatability, and validity of ALP volumetric measures were previously reported.27 ALP gray matter volumetric measures of the right hippocampus were obtained by two different operators on the same group of 43 brain MRI randomly selected from the entire CHS dataset: mean volumes were 4.8824 versus 4.85347 cm3 (mean % difference: 0.6%, P = 8.5−16 ). The intraclass correlation coefficient of volumes obtained from ALP versus handtracing method was 0.99 (95% CI: 0.25-0.99), indicating overlapping volumes. Compared to AIR or SPM, the fully deformable registration used by ALP produced automated segmentations with higher agreement with manual segmentations (t (9)= –5.2, P < 0.0006) 29 and with fewer intersubject registration,30 indicating that ALP can measure ROIs volumes more accurately than AIR or SPM. As part of quality control, each image was inspected for large structural abnormalities (eg, strokes or hematomas) that would deform the brain shapes and interfere with accuracy of volumetric measures. Each image was aligned to the AC-PC line to facilitate the spatial normalization process. MTL gray matter volume was computed as the sum of the gray matter volumes of its anatomical subcomponents (hippocampus, amygdala, and parahippocampus, see Fig 1A) for both the right and left hemispheres. The gray matter volume of the whole brain and total brain volume were also obtained using ALP. Total brain volume was calculated as the sum of voxel counts from the gray matter, the white matter, and the cerebrospinal fluid of the whole brain. MTL volume as a percentage of total brain volume was used for these analyses. Covariates
The following measures were obtained concurrently with the time of the MR scan: age, years of education, 3MSE scores, and the presence of cardiovascular disease31 (physician diagnosis of myocardial infarction, angina, coronary artery bypass surgery or percutaneous transluminal coronary angioplasty, congestive heart failure, stroke or transient ischemic attack, or intermittent claudication). Gender and race were obtained from the initial visit in 1989. The presence of the APOe4 allele was also considered as a covariate in those participants who gave consent for the use of their DNA (n = 151 out of n = 155). Head size, total brain volume, and ventricular enlargement were also included in the model. Statistical Analysis As noted above, by the end of follow-up 116 remained cognitively normal, 43 converted to MCI, and 39 to AD. Because the date of onset for these outcomes were
Rosano et al: Predictors of Conversion to AD
151
approximate for AD and not available for MCI cases, we analyzed these data as a case-control study of cognitively normal versus AD cases, and we therefore included n = 155 participants in this analysis. Characteristics of the analytical sample of n = 155 are in Table 2. The distribution of demographics (age, race, and education) and the prevalence of risk factors (Allele 4 ApoE, coronary heart disease, diabetes, stroke) were compared between the two groups. Mean volumetric measures were computed separately for each hemisphere, and one-way analyses of variance (ANOVAs) were used to compare these values across the two groups, and analysis of covariance (ANCOVA) was used to test for mean difference after adjusting for head size and total brain volume. The data were analyzed longitudinally using logistic regression models. In preliminary analysis, volumetric measures were used both as continuous and discrete (tertiles) variables, with the largest tertile considered as the reference group. In order to analyze whether MTL volumes and cerebrovascular disease were independently associated with conversion to AD, we examined the change in odds ratios (ORs) associated with each of these variables (MTL volume, WMH ≥ grade 4, and the presence of at least 1 brain infarct) as they were added to the same model, and also after adjusting for covariates. To examine the combined effect of smaller MTL volume and burden of WMH (see Fig 1), a new ordinal variable consisting of four groups was created, based on whether participants had a small (eg, were in the 1st tertile) versus large (2nd or 3rd tertile) MTL volume and had WMH ≥ grade 4 or <4. These were coded as dummy variables in the logistic models, with the group at lowest risk (“large MTL and WMH < grade 4”) used as reference group. Similarly, a 4-level ordinal variable was created for those with a small versus large MTL volume with presence versus absence of at least 1 subclinical brain infarct. This was also coded as dummy, with the group at lowest risk (“large MTL and no subclinical brain infarcts”) used as reference group.
Results Older adults converting to AD were older (P = 0.03), more likely to be women (P = 0.04), to have a smaller MTL (P < 0.0001 for both hemispheres), and to have at least 1 brain infarct (P = 0.03) compared to those remaining cognitively normal (see Table 2). Compared to the rest of the group, those converting to AD were also more likely to be positive for APOe4 allele (P = 0.08), to have coronary heart disease (P = 0.2) and to have WMH ≥ grade 4 (P = 0.3), although these differences were not significant. Mean difference in MTL volume remained
152
Journal of Neuroimaging Vol 17 No 2 April 2007
Table 3.
Odds Ratios (OR) and 95% Confidence Intervals (CI) from Multivariate Logistic Regression Models for Risk to Develop Alzheimer’s Disease (AD)
Independent Variables
Predictors Left MTL (% of total brain volume), tertiles 3 (>0.9%) 2 (0.8-0.9%) 1 (<0.8%) White matter hyperintensity ≥ grade 4 Subclinical brain infarcts ≥1∗ Covariates Age (yrs) Female gender White race Education (yrs) 3MSE score >95 Presence of APOe4 allele Head size†
Outcome: Conversion to AD
Adjusted OR and 95% CI 1.0 3.2 (1.1, 9.0) 4.4 (1.5, 12.3) 0.8 (0.3, 2.8) 2.7 (1.0, 7.1) 1.1 (1.0,1.3) 0.9 (0.3, 2.6) 0.7 (0.2, 2.4) 0.9 (0.4, 2.1) 1.2 (0.5, 2.9) 2.8 (1.0, 7.1) 0.6 (0.3, 1.2)
Further adjustment for estimated time of onset changed the coefficients by 4%. ∗ When basal ganglia >1 were in the model, OR (95% CI): 3.5 (1.1, 10.9). † Adding head size to the model changed the regression coefficients by less than 4%.
significant after adjusting for head size (left: P = 0.002, right: P = 0.003). Those in the lowest tertile of left MTL volume had a greater risk to convert to AD compared to those in the highest tertile, independent of other covariates (see Table 3). Adding covariates to the model changed the regression coefficients by less than 5%. The presence of one or more subclinical brain infarcts was also significantly associated with risk of conversion to AD independent of covariates, total brain volume, and MTL volume. Results were similar for lacunar infarcts. In the fully adjusted model, severity of WMH (WMH ≥ grade 4) was not an independent predictor of risk of conversion to AD, and the only 2 other variables significantly associated with AD-conversion risk were age and presence of APOe4 allele. The interaction between MTL volumes and APOe4, 3MSE (≥ 95) or total brain volume were not significant. Results were similar when MTL volume was used as a continuous variable. The combined effect of MTL atrophy and cerebrovascular disease on risk of AD conversion is reported in Table 4. Those with WMH ≥ grade 4 and a small MTL (eg, those in the first tertile) had a more than three times greater risk of conversion to AD compared to those with WMH < grade 4 and a large MTL (eg, in the 2nd or 3rd
Table 4.
Odds Ratios (OR) and 95% CI from Three Separate Multivariate Logistic Regression Models for Risk to Develop Alzheimer’s Disease (AD)
Independent Variable
N
Risk of AD Conversion OR (95% CI)
Co-occurrence of MTL atrophy† and of WMH WMH< grade 4 and large MTL 95 1.0 WMH< grade 4 and small MTL 35 1.1 (0.3, 4.9) WMH≥ grade 4 and large MTL 15 2.2 (0.8, 5.6) WMH≥ grade 4 and small MTL 10 3.6 (0.8, 17.1) Co-occurrence of MTL atrophy† and of subclinical brain infarcts (BI) BI = 0 and large MTL 84 1.0 BI = 0 and small MTL 30 2.4 (0.9, 7.8) BI ≥1 and large MTL 25 2.6 (0.9, 7.8) BI ≥1 and small MTL 16 7.0 (1.5, 33.1) Co-occurrence of MTL atrophy† and of basal ganglia infarcts (BgI) BgI = 0 and large MTL 91 1.0 BgI = 0 and small MTL 37 2.6 (1.0, 6.7) BgI >1 and large MTL 19 3.2 (1.0, 10.7) BgI > 1 and small MTL 9 6.7 (1.6, 40.4) Model adjusted for age, race, gender, education, baseline 3MS score, APOe;4 allele, head size. MTL = medial temporal lobe; WMH = white matter hyperintensities; BI = subclinical brain infarcts; BgI = subclinical basal ganglia infarcts. † Medial temporal lobe volume was computed as % of total brain volume. “Small”: 1st tertile, “Large”: 3rd tertile.
tertile), but associations were not significant. In contrast, a 7-fold significant increase in the risk of AD conversion was found among those with at least 1 brain infarct, or with one infarct in the basal ganglia, who also were in the lowest tertile of MTL. In these models, none of the other covariates was significantly associated with risk of conversion, with the exception of a very marginal association between APOe4 allele and risk of AD conversion (OR [95% CI], P -value: 2.5 [1.0, 6.3], P = 0.05). Analyses were repeated after exclusion of the 4 participants with mixed AD-Vascular Dementia and yielded similar results. Results were also similar for those converting to Probable AD versus Possible AD. Similar results were also obtained when using the Cox proportional hazard model. Discussion This study contributes to our understanding of the importance of co-occurrence of cerebrovascular disease and focal atrophic processes for the risk of conversion to AD among cognitively normal older adults. We showed that in cognitively normal older adults, the combination of
MTL atrophy and of subclinical brain infarcts is associated with a 7-fold increase in the risk to develop AD over time. These associations were not explained by age, education, genetic risk factors or 3MSE, or by presence of global brain abnormalities, such as smaller total brain volume or ventricular enlargement. While the small sample size of the groups with cerebrovascular diseases and small MTL limited the statistical power, the consistently large risk estimates of this study warrant further studies with larger sample sizes, and in particular with more individuals with WMH or subcortical lacunar infarcts. These results have direct clinical relevance, as older adults often have MRI signs of cerebrovascular disease in the absence of clear cognitive deficits. The additional presence of a smaller MTL may represent a useful and simple tool to discriminate those cognitively normal older who have a greater risk of conversion to AD. These measures can be easily measured from a brain MRI obtained at one single point in time, and they can provide risk estimates that are significant independently of other individual’s characteristics and most importantly—of APOe4 genotype. Most important is the fact that, among the various factors that can increase risk of AD, cerebrovascular disease is the one that can be modified.32,33 Antihypertensive treatments may stop or delay progression of subclinical cerebral disease, suggesting the possibility that, in addition to modifying the risk of developing agerelated cognitive impairment,34,35 control of cardiovascular risk factors could also reduce the risk to convert to AD. Consistent with other studies,11,36-38 we found that severity of WMH was not significantly associated with the risk of AD conversion, once focal or total gray matter volume were accounted for. The difference between our findings and those of former studies on the association between WMH and cognitive impairment12,15,39,40 may be explained by the fact that in other studies the statistical models were not adjusted for measures of focal or total gray matter volume or head size. It is possible that these semiquantitative unadjusted measures of global and diffuse WMH indicate age-related-, rather than diseasespecific, brain morphological changes. Quantitative studies examining the spatial distribution of WMH in specific tracts of interest for cognitive function, such as the latemyelinating neocortical regions,41 may discern the direct contribution of WMH to AD risk. We found a strikingly consistent lateralization of dementia risk within the left hemisphere. Others42,43 have also shown that risk of dementia is greater for those with accelerated gray matter loss in the left hemisphere. A
Rosano et al: Predictors of Conversion to AD
153
greater susceptibility of the left hemisphere versus the right hemisphere to the process of aging is known. The reasons for this lateralization are still under investigation. Perhaps AD pathology is overlaying on the age-related brain shrinkage and the lateralization that we observe is in fact a result of aging, not of AD. We noticed that small lacunar infarcts, mostly located in the basal ganglia, had similarly strong association with AD risk compared with large cortical infarcts. These lacunar infarcts could impair the basal lentiform/striatum circuitry, which is crucial for executive functions and which is affected in AD. Future studies will need to assess whether there is a change in the structure/volume of these subcortical areas associated with AD. Mungas and colleagues have shown that changes in lacunar infarcts, but not baseline lacunar infarcts, are associated with cognitive decline independently of focal volumes and of WMH.37-39 Although the outcomes of these studies were the change in global cognition score or in various individual cognitive tests rather than conversion to AD, their findings support the importance of looking at this specific cerebrovascular marker in association with cognitive function. Our results need to be replicated in a larger population, and the ALP volumetric method employed here is an ideal candidate to quickly and reliably assess neuroanatomical correlates of dementia risk in large epidemiological studies. It is fully automated, and it provides individual volumetric measures of individual regions of interest. Other strengths of this study include the large number of cognitively normal adults at baseline, the availability of focal and global markers of brain disease, a thorough examination of neurological data and the wealth of information on cardiovascular diseases and associated risk factors. However, we did not include measures of new cerebrovascular events in the model, and these may explain some of the dementia cases above and beyond the presence of smaller brain volumes and subclinical cerebrovascular disease. This longitudinal analysis of a large group of cognitively normal older adults provided dementia risk estimates associated with specific brain volumetric measures in the presence of markers of diffuse and subclinical cerebrovascular brain disease. Understanding the interrelationship between cerebrovascular disease and AD-related focal atrophy may provide insights into preventive strategies and quantitative tools to monitor pharmacological treatment outcomes. Automated morphometric techniques providing volumetric measures of brain regions may offer a critical index of dementia risk, especially when accompanied by signs of subclinical cerebrovascular disease.
154
Journal of Neuroimaging Vol 17 No 2 April 2007
Disclosure The authors do not have personal financial relationships and they all report that they have no conflicts of interest. The research reported in this article was supported by Claude Pepper Center and by contracts T32 AG00181-11, R01AGO15928, R01AG020098, N01-HC-85079 through N01-HC-85086, N01-HC35129, and N01 HC-15103 from the National Heart, Lung, and Blood Institute. A full list of participating CHS investigators and institutions can be found at http://www.chs-nhlbi.org. The authors wish to thank Mr. R. Crooks and Ms J. Cochran for their contribution to data processing and Mrs. M. Nable for her help with manuscript preparation.
References 1. Kuller LH, Lopez OL, et al. Risk factors for dementia in the cardiovascular health cognition study. Neuroepidemiology 2003;22:13-22. 2. Scheltens P, Korf ES. Contribution of neuroimaging in the diagnosis of Alzheimer’s disease and other dementias. Curr Opin Neurobiol 2000;13:391-396. 3. De Leon MJ, DeSanti S, et al. MRI and CSF studies in the early diagnosis of Alzheimer’s disease. J Intern Med 2004;256:205-223. 4. Chetelat G, Baron JC. Early diagnosis of Alzheimer’s disease: contribution of structural neuroimaging. Neuroimage 2003;18:525-541. 5. Erkinjuntti T, Lee DH, et al. Temporal lobe atrophy on magnetic resonance imaging in the diagnosis of early Alzheimer’s disease. Arch Neurol 1993;50:305-310. 6. Braak H, Braak E, et al. Staging of Alzheimer-related cortical destruction. Eur Neurol 1993;33:403-408. 7. Thompson PM, Hayashi KM, et al. Dynamics of gray matter loss in Alzheimer’s disease. J Neurosci 2003;23:994-1005. 8. Baron JC, Chetelat G, et al. In vivo mapping of gray matter loss with voxel-based morphometry in mild Alzheimer’s disease. Neuroimage 2001;14:298-309. 9. Stoub TR, Bulgakova M, et al. MRI predictors of risk of incident Alzheimer disease: a longitudinal study. Neurology 2005;64:1520-1524. 10. Convit A, de Asis J, et al. Atrophy of the medial occipitotemporal, inferior, and middle temporal gyri in nondemented elderly predict decline to Alzheimer’s disease. Neurobiol Aging 2000;21:19-26. 11. Schmidt R, Ropele S, et al. White matter lesion progression, brain atrophy, and cognitive decline: the Austrian stroke prevention study. Ann Neurol 2005;58:610-616. 12. Kuller LH, Lopez OL, et al. Risk factors for dementia in the cardiovascular health cognition study. Neuroepidemiology 2003;22:13-22. 13. den Heijer T, Geerlings MI, et al. Use of hippocampal and amygdalar volumes on magnetic resonance imaging to predict dementia in cognitively intact elderly people. Arch Gen Psychiatry 2006;63:57-62. 14. van der Flier WM, van Straaten EC, et al. LADIS study group. Medial temporal lobe atrophy and white matter hyperintensities are associated with mild cognitive deficits in non-disabled elderly people: the LADIS study. J Neurol Neurosurg Psychiatry 2005;76:1497-1500.
15. Wu CC, Mungas D, et al. Brain structure and cognition in a community sample of elderly Latinos. Neurology 2002;59:383-391. 16. van der Flier WM, Middlekoop HA, et al. Interaction of medial temporal lobe atrophy and white matter hyperintensities in AD. Neurology 2004;62:1862-1864. 17. Fried LP, Borhani NO, et al. The Cardiovascular Health Study: design and rationale. Ann Epidemiol 1991;1:263-276. 18. Lopez OL, Kuller LH, et al. Evaluations of AD in the cardiovascular health cognition study. Neuroepidemiology 2003;22:1-12. 19. Lopez OL, Kuller LH, et al. Classification of vascular dementia in the Cardiovascular Health Study Cognition Study. Neurology 2005;64:1539-1547. 20. Lopez OL, Jagust WJ, et al. Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study Cognition Study: part 1. Arch Neurol 2003;60:13851389. 21. Teng EL, Chui HC. The Modified Mini-Mental State (3MS) examination. J Clin Psychiatry 1987;48:314-318. 22. McKhann G, Drachman D, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984;34:939-944. 23. Xu WL, Qui CX, Wahlin A, Winblad B, Fratiglioni L. Diabetes mellitus and risk of dementia in the Kungsholmen project: a 6-year follow-up study. Neurology 2004;63:11811186. 24. Moroney JT, Tang M-X, Berglund L, et al. Low-density lipoprotein cholesterol and the risk of dementia with stroke. JAMA 1999;282:254-260. 25. Bryan RN, Manolio TA, et al. A method for using MR to evaluate the effects of cardiovascular disease on the brain: the cardiovascular health study. AJNR Am J Neuroradiol 1994;15:1625-1633. 26. Yue NC, Arnold AM, et al. Sulcal, ventricular, and white matter changes at MR imaging in the aging brain: data from the cardiovascular health study. Radiology 1997;202:3339. 27. Rosano C, Becker J, et al. Morphometric analysis of gray matter volume in demented older adults: exploratory analysis of the cardiovascular health study brain MRI database. Neuroepidemiology 2005;24:221-229. 28. Tzourio-Mazoyer N, Landeau B, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002;15:273-289. 29. Carmichael OT, Aizenstein HJ, et al. Atlas-based hip-
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
pocampus segmentation in Alzheimer’s disease and mild cognitive impairment. Neuroimage 2005;27:979-990. Wu M, Carmichael O, et al. Quantitative comparison of AIR, SPM, and fully deformable registration for atlas-based segmentation of functional and structural MR Images 2006. Hum. Brain Map. 27(9):747-754. Ives DG, Fitzpatrick AL, et al. Surveillance and ascertainment of cardiovascular events. The Cardiovascular Health Study. Ann Epidemiol 1995;5:278-285. Dufouil C, Chalmers J, et al. Effects of blood pressure lowering on cerebral white matter hyperintensities in patients with stroke: the PROGRESS (perindopril protection against recurrent stroke study) Magnetic Resonance Imaging Substudy. Circulation 2005;112:1644-1650. de Leeuw FE, De Groot CJ, et al. Hypertension and cerebral white matter lesions in a prospective cohort study. Brain 2002;125:765-772. Waldstein SR, Giggey PP, et al. Nonlinear relations of blood pressure to cognitive function: the Baltimore Longitudinal Study of Aging. Hypertension 2005;45:374-379. Forette FM, Seux ML, et al. Prevention of dementia in randomized double-blind placebo-controlled Systolic Hypertension in Europe (Syst-Eur) trial. Lancet 1998;52(9137):1347-1351. Bigler ED, Kerr B, et al. White matter lesions, quantitative magnetic resonance imaging, and dementia. Alzheimer Dis Assoc Disord 2002;16:161-170. Mungas D, Reed BR, et al. Volumetric MRI predicts rate of cognitive decline related to AD and cerebrovascular disease. Neurology 2002;59:867-873. Mungas D, Harvey D, et al. Longitudinal volumetric MRI change and rate of cognitive decline. Neurology 2005;65:565-571. Mungas D, et al. MRI predictors of cognition in subcortical ischemic vascular disease and Alzheimer’s disease. Neurology 2001;57:2229-2235. van der Flier WM, van Straaten EC, et al. Small vessel disease and general cognitive function in nondisabled elderly: the LADIS study. Stroke 2005;36:2116-2120. Bartzokis G. Age-related myelin breakdown: a developmental model of cognitive decline and Alzheimer’s disease. Neurobiol Aging 2004;25:5-18. Thompson PMHK, De Zubicaray GI, et al. Mapping hippocampal and ventricular change in Alzheimer disease. Neuroimage 2004;22:1754-1766. Bell-Mc Ginty S, Lopez OL, Meltzer CC, Scanlon JM, Whyte EM, Dekosky ST, Becker JT. Differential cortical atrophy in subgroups of mild cognitive impairment. Arch Neurol 2005;62:1393-1397.
Rosano et al: Predictors of Conversion to AD
155