ORIGINAL ARTICLE
Is it a (fe)male pain? Portuguese nurses’ and laypeople’s gendered representations of common pains S.F. Bernardes1,2, S.A. Silva1,3, H. Carvalho1,4, M. Costa1, S. Pereira1 1 2 3 4
Instituto Universitário de Lisboa (ISCTE-IUL), Lisbon, Portugal Centro de Investigação e Intervenção Social (Cis-IUL), Lisbon, Portugal Business Research Unit (Bru-IUL), Lisbon, Portugal Centro de Investigação e Estudos de Sociologia (Cies-IUL), Lisbon, Portugal
Correspondence Sónia F. Bernardes E-mail:
[email protected] Funding sources This research was funded by Fundação para a Ciência e Tecnologia (PTDC/PSI-PSO/099809/2008). Conflicts of interest None declared. Accepted for publication 22 July 2013 doi:10.1002/j.1532-2149.2013.00387.x
Abstract Background: Although many studies have explored gender role expectations of pain behaviours in different cultures, only a few authors have tried to explore whether certain pains are more associated with the typical man or woman. Hence, this study aimed at exploring, among Portuguese laypeople and nurses, patterns of common pains more strongly associated with the typical man or woman, and their relationship with health-care training and personal pain experiences. Methods: A total of 68 nurses (76% women) and 55 laypeople (62% women) were asked to identify, through free association, the most frequent common pains that people in general associate with the typical man and woman, respectively, and also to report their personal past pain experiences. A content analysis was used to categorize and quantify participants’ responses. A multiple correspondence analysis was performed to identify gendered patterns of common pains, followed by a cluster analysis to classify participants according to their endorsed patterns. Results: Findings showed that while ‘back and musculoskeletal pains’ was the only pattern associated with the typical man, more differentiated patterns of pains were associated with the typical woman, namely (1) headaches; (2) abdominal, back and musculoskeletal pains; and (3) pains due to hormonal cycles, labour/puerperium and from the urinary/ reproductive system. These representations were shared by laypeople and nurses and were only significantly associated with personal experiences of pains from the urinary/reproductive system. Conclusions: This study identified different gendered patterns of common pains, which may have important implications for (wo)men’s pain experiences and how these are interpreted by others.
1. Introduction Are there any typically (fe)male common pains? In many cultures, most people expect men and women to show different pain thresholds, tolerance levels, willingness to report pain or pain coping strategies (Robinson et al., 2001; Keogh and Denford, 2009; Defrin et al., 2011; Alabas et al., 2012). These genderrole expectations of pain partially account for sex530 Eur J Pain 18 (2014) 530–539
related differences in pain experiences (Robinson et al., 2003a; Alabas et al., 2012) and assessments (Robinson and Wise, 2003). However, few authors have tried to explore whether there are common pains (as opposed to pain behaviours) more strongly associated with gender stereotypes, i.e., gendered common pains. This paper contributes to bridging this gap. Gendered representations of common pains may influence men’s and women’s pain experiences and © 2013 European Pain Federation - EFIC®
S.F. Bernardes et al.
What’s already known about this topic? • Few studies have explored whether certain pain events are more associated with the typical (wo)man. • American college students reported childbirth/ menstrual cycle and injury, respectively, as the ‘worst pain imaginable’ for the typical (wo)man. What does this study add? • This study goes beyond previous findings by differentiating more complex gendered patterns of common pains and exploring their association with health-care training and personal past pain experiences, in a (more heterogeneous) sample of Portuguese laypeople and nurses.
how these are interpreted by others. For example, due to the higher prevalence of fibromyalgia among women, doctors are reluctant to provide this diagnosis to male patients and the latter report feeling profound shame when they receive it (Paulson et al., 1999, 2002). Therefore, exploring the gendered nature of common pains seems a relevant research goal. To the best of our knowledge, only two studies, conducted by Robinson et al. (2003b, 2004), have directly approached this issue. American college students were asked for an event, medical condition or injury associated with the worst pain imaginable for the typical man and woman. Regardless of participants’ sex, the painful events more associated with the typical woman were childbirth and the menstrual cycle, while injury was the event most associated with the typical man. Such studies, however, have some shortcomings. First, by asking participants to report painful events associated with the worst pain imaginable, the authors have constrained participants’ discourses to pain aetiology and, more precisely, to extreme (as opposed to common) pain events. It would also be interesting to explore whether more common pains and also other dimensions of pain experiences (e.g., pain location/ system, severity, quality) might have gender connotations. Moreover, whether there are any identifiable gendered patterns/representations of common pains is a question that remains unanswered. Second, the findings are difficult to generalize to samples of participants within other age ranges, from other cultural backgrounds and/or with health-care training. This latter aspect seems particularly relevant, given that the extent to which health-care professionals share with laypeople the same gendered representations of © 2013 European Pain Federation - EFIC®
Is it a (fe)male pain?
common pains might have important implications for pain management. Finally, while previous pain experiences have been found to be associated with the most intense self-imagined pain (Robinson et al., 2004), choice of pain anchors (Dannecker et al., 2007) or accuracy in rating another person’s pain (Robinson and Wise, 2004), the extent to which past pain experiences are associated with an individual’s gendered representations of common pains seems yet to be ascertained. To resolve these shortcomings, the aims of this study were to explore, among Portuguese laypeople and nurses, (1) patterns of common pains more strongly associated with the typical man or woman and (2) whether health-care training and personal past pain experiences are associated with these gendered patterns of common pains.
2. Methods 2.1 Participants This study had a convenience sample of 68 nurses (76% women) and 55 laypeople (62% women). Nurses’ ages ranged from 24 to 50 years old (M = 36.63; SD = 6.32). They worked in several hospital services (e.g., Oncology, Intensive Care Units, Emergency Rooms, Cardiology, Surgery), with 1–30 years of professional experience (M = 13.97; SD = 6.11). Around 22% of the nurses (14 women and 1 man) reported suffering or having suffered constant or intermittent pain for more than 3 months, mostly on a daily or weekly basis, with an average intensity of 5.38 out of 10 (SD = 2.02). Also, 75% of them reported having frequent professional contact with chronic pain (CP) patients (M = 5.15 out of 7; SD = 1.24) and 60% were acquainted with other persons suffering from CP, mostly family members. Laypeople’s ages ranged from 20 to 49 years old (M = 30.98, SD = 8.68); 95% had higher education degrees in one of several scientific domains (e.g., Law, Management, Marketing, Psychology, Sociology). Around 35% of these participants (13 women and 6 men) reported suffering or having suffered constant or intermittent pain for more than 3 months, again mostly on a daily or weekly basis, with an average intensity of 6.11 out of 10 (SD = 1.78). The majority of these participants (78%) knew people who suffered or had suffered from CP. Age was the only significant difference found between nurses and laypeople, t (96.23) = −4.026; p < 0.001.
2.2 Instrument Data were collected using a questionnaire elaborated for the purpose and based on a free association methodology commonly used to explore and identify stereotype content (e.g., Amâncio, 1994; Augoustinos and Ahrens, 1994; Krueger,
Eur J Pain 18 (2014) 530–539
531
Is it a (fe)male pain?
1996). The questionnaire consisted of three open-ended questions. Participants were asked to answer, by free association, the first two questions, which were designed to identify the most frequent common pains associated with the typical man and woman, respectively: ‘Throughout their lives, most people feel pain once in a while. Please report some pains that people in general associate to the typical (wo)man.’ The order of presentation of these two questions was counterbalanced. The third question asked participants to report some personal past pain experiences. Finally, sociodemographic data and information pertaining to personal and vicarious experiences with CP were collected.
2.3 Design In this study, a mixed methodology was used combining a qualitative approach with a quasi-experimental design. The qualitative approach entailed a content analysis of participants’ answers. The quasi-experimental design was betweensubjects: 2 (participants’ sex) × 2 (health-care training: present vs. absent, i.e., nurses vs. laypeople) × 2 (order of presentation of the first two questions of the aforementioned instrument). Taking in consideration our mixed design, we decided a priori to include around 30 individuals per condition (excluding the control variable ‘order of presentation’) in order to provide the conditions for (1) theoretical saturation (e.g. Flick, 2007) and (2) running parametric tests if needed.
2.4 Procedure This study was approved by the Institutional Review Board of the Centro de Investigação e Intervenção Social. The questionnaires were administered to small groups of participants while they were attending post-graduation classes or training sessions. The participants were invited to collaborate on a study on how people perceive pain events. After participants verbally consented to collaborate, they were given the questionnaires without any other specific instructions. Time of completion of the questionnaires ranged from 5 to 10 min.
2.5 Data analyses Participants’ answers were submitted to a content analysis based on Saldaña’s (2009) proposed procedures and supported by ATLAS.ti 6.2 (Muhr, 2004). A semantic segmentation of the data was used and conceptual categories were developed by a mixed process, i.e., either by bottom-up or top-down processes (Saldaña, 2009; see all conceptual categories in Table 1). The development of some of the major conceptual categories (e.g., Region, System, and Aetiology) was based on the axes of the International Association for the Study of Pain Scheme for Coding CP Diagnosis (Merskey and Bogduk, 1994). The category ‘Sensory Quality of Pain’ was adapted from the Portuguese version of the McGill Pain
532 Eur J Pain 18 (2014) 530–539
S.F. Bernardes et al.
Questionnaire (Pimenta and Teixeira, 1996). All the remaining conceptual (sub)categories were developed through a bottom-up process. The final category system included six major conceptual categories, which encompassed 34 subcategories (Table 1). It should be noted that due to the nature of the data, most units of analysis (e.g., headache) could be assigned to several conceptual (sub)categories (e.g., nature/ physical, region/head); hence, these were not mutually exclusive. Finally, data codification was supported by a category dictionary, which included the name and definition of each (sub)category along with examples of associated units of analysis. In order to test the reliability of the conceptual category system, we randomly selected 100 units of analysis that were separately coded by three independent judges, who were given the category dictionary. Krippendorff’s alpha (Hayes and Krippendorff, 2007) was used and calculated separately for each major conceptual category (see Table 1). Generally, results showed overall good reliability indices, with one exception (0.74), which is still considered acceptable. Afterwards, participants’ answers were quantified according to the presence or absence of the conceptual subcategories (0 = not mentioned; 1 = mentioned). Table 1 shows the proportion of participants who mentioned each conceptual subcategory for the typical man/woman and for the self. Only the conceptual subcategories that were mentioned by at least 15% of the overall participants (highlighted in bold in Table 1) were included in further analyses and considered for interpretation purposes. Given the absence of a gold standard criterion, the decision on this cut-off value was based on the need to achieve a balance between two criteria: (1) avoiding residual (sub)categories that could be problematic when running the multiple correspondence analysis (MCA) and (2) retaining (sub)categories that were conceptually relevant to our research. Also, because the order of presentation of the first two answers of the questionnaire did not show any significant effects on the proportion of reported pains for the typical man/woman and the self (p > 0.001), this variable was not considered in the analyses that follow. Chi-square analyses were conducted to explore the effects of participants’ sex and health-care training on pains more associated with the typical man or woman, and on pain self-reports. Afterwards, in order to identify patterns of common pains more associated with the typical woman or the typical man, an MCA was performed using the conceptual subcategories highlighted for the typical woman and typical man in Table 1 as active variables (Fig. 1). MCA is a multivariate method used to explore interrelationships between multiple categorical variables (Greenacre, 2007; Carvalho, 2008; Ramos and Carvalho, 2011). Like principal components analysis (PCA), MCA generates a set of factorial dimensions that summarize the associations between those categorical variables. Also, as in PCA, where the interpretation of the resulting components is based on the variables’ loadings, in the MCA, the interpretation of the dimensions is based on the discrimina-
© 2013 European Pain Federation - EFIC®
S.F. Bernardes et al.
Is it a (fe)male pain?
Table 1 Frequency and proportion of participants mentioning each subcategory for the typical (wo)man and the self. Pain self-reports
(Sub)Categories Regions (α = 0.93) Head Back Abdominals Teeth Lower limbs Ears Chest Throat Upper limbs Genitalia Breast Systems (α = 0.84) Musculoskeletal Urinary/Reproductive Digestive Respiratory/Circulatory Nervous Aetiology (α = 0.87) Hormonal cycles Labour/Puerperium Psychological Growth Trauma/Injury Chronic illness Acute disease Effort Nature (α = 0.74) Physical Psychological Sensory properties (α = 0.95) Tingling Stabbing Sore Spasmodic Diffuse Thermal Duration (α = 0.79) Chronic Acute
Typical man (N = 123) n (%)
Typical woman (N = 123) n (%)
Men (N = 37) n (%)
Women (N = 86) n (%)
29 (23.6) 51 (41.5) 9 (7.3) 12 (9.8) 9 (7.3) 1 (0.8) 6 (4.9) 2 (1.6) 3 (2.4) 2 (1.6) 0
88 (71.5) 22 (17.9) 21 (17.1) 8 (6.5) 11 (8.9) 1 (0.8) 3 (2.4) 1 (0.8) 2 (1.6) 2 (1.6) 0
19 (51.4) 10 (27.0) 11 (29.7) 23 (35.1) 1 (2.7) 3 (8.1) 2 (5.4) 1 (2.7) 0 0 0
55 (64.0) 30 (34.9) 17 (19.8) 17 (19.8) 6 (7.0) 9 (10.5) 2 (2.3) 2 (2.3) 2 (2.3) 0 3 (3.5)
59 (48.0) 6 (4.9) 8 (6.5) 9 (7.3) 2 (1.6)
20 (16.3) 84 (68.3) 5 (4.1) 3 (2.4) 2 (1.6)
13 (35.1) 2 (5.4) 6 (16.2) 3 (8.1) 0
19 (22.1) 28 (32.6)a 8 (9.3) 3 (3.5) 1 (1.2)
0 0 1 (0.8) 1 (0.8) 6 (4.9) 5 (4.2) 4 (3.3) 8 (6.5)
71 (57.7) 33 (26.8) 2 (1.6) 1 (0.8) 1 (0.8) 5 (4.1) 3 (2.4) 2 (1.6)
0 0 0 0 3 (8.1) 1 (2.7) 3 (8.1) 3 (8.1)
20 (23.3) 7 (8.1) 1 (1.2) 0 4 (4.7) 1 (1.2) 4 (4.7) 3 (3.5)
108 (87.8) 15 (12.2)
116 (94.3) 22 (17.9)
36 (97.3) 5 (13.5)
78 (90.7) 15 (17.4)
0 3 (2.4) 2 (1.6) 3 (2.4) 1 (0.8) 2 (1.6)
0 0 5 (4.1) 5 (4.1) 1 (0.8) 0
0 0 0 2 (5.4) 0 0
1 (1.2) 2 (2.3) 2 (2.3) 6 (7.0) 0 0
4 (3.3) 9 (7.3)
4 (3.3) 3 (2.4)
0 2 (5.4)
0 5 (5.8)
Note: Values in bold are above the cut-off value (15%). a Significant sex-related differences in pain self-reports (p ≤ 0.001).
tion measures and the contributions of the active variables (see Table 2). The most relevant active variables for each dimension are the ones that have the highest discrimination/ contributions values (i.e., highest explained variance). Moreover, MCA provides a graphical display of the structure of the associations between all the categories into a subspace that has the fewest dimensions as possible, like the bidimensional graph presented in Fig. 1. The groups/patterns are identified by considering the associations between the cat-
© 2013 European Pain Federation - EFIC®
egories with the highest contributions to one or both factorial dimensions, i.e., the geometrical proximity of the categories in the factorial plane. Next, a hierarchical cluster analysis (HCA; Hair et al., 2010; Mooi and Sarstedt, 2011) was performed in order to validate the MCA pattern solution, using MCA standardized object scores in the two dimensions as input variables. The HCA was suited by a k-means algorithm (non-hierarchical clustering method on the basis of an overall optimization
Eur J Pain 18 (2014) 530–539
533
Is it a (fe)male pain?
S.F. Bernardes et al.
testing relations (chi-square analyses and analysis of variance) with the identified clusters. All statistical analyses were performed with the support of IBM SPSS Statistics (version 20, International Business Machines Corp. Armonk, NY, USA). It should also be noted that due to the considerable amount of analyses, in order to prevent for an inflated type I error, we considered a Bonferroni correction that reduced our critical value to p ≤ 0.001.
3. Results 3.1 (Patterns of) gendered common pains
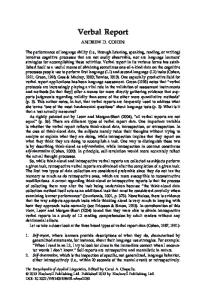
Note: Lined squares = patterns/representations of common pains; dashed squares = clusters of participants; TM = typical man; TW = typical woman; only the “mentioned” (vs. “not mentioned”) answer categories are visible.
Figure 1 Topological configuration of the gendered patterns of common pains and the projection of clusters.
criterion) and clusters of participants were identified according to their own pattern (Fig. 1). Finally, health-care training (nurses vs. laypeople), participants’ sex and age, personal CP and past common pain experiences (present vs. absent) were later considered for
Our first goal was to identify (patterns of) common pains that were more strongly associated with the typical man or woman. For the typical man, Table 1 shows that the two pain regions most frequently mentioned were back and head, although the former showed a higher consensus than the latter. Almost half of the participants mentioned musculoskeletal pain, while the remaining systems were rarely reported. Almost all participants mentioned pain of physical nature and also, but to a much lesser extent, psychological pain. Although very low proportions of participants mentioned pain aetiology for the typical man, it should be noted that effort and trauma/injury were still the two most mentioned subcategories. Regarding the typical woman, almost three quarters of the sample reported pain in the head. Back and abdominal pains were also mentioned but in a much lower proportion. The majority of participants men-
Table 2 Discrimination measures of the variables entered in the multiple correspondence analysis. Dimensions 1
2
Variables
Discrimination
Contribution (%)
Discrimination
Contribution (%)
Head – TM Head – TW Back – TM Back – TW Abdominals – TM Abdominals – TW Musculoskeletal – TM Musculoskeletal – TW Urinary/Reproductive system – TM Urinary/Reproductive system – TW Hormonal cycles – TW Labour/Puerperium – TW Psychological nature – TM Psychological nature – TW Active total Inertia
0.096 0.430 0.219 0.152 0.012 0.000 0.228 0.101 0.001 0.442 0.408 0.036 0.509 0.468 3.103 0.222
3.11 13.87 7.04 4.91 0.39 0.00 7.35 3.24 0.03 14.25 13.14 1.18 16.41 15.08 100.00
0.007 0.054 0.066 0.181 0.030 0.379 0.033 0.107 0.007 0.376 0.263 0.357 0.009 0.045 1.914 0.137
0.39 2.81 3.43 9.45 1.57 19.82 1.72 5.59 0.36 19.64 13.73 18.67 0.45 2.37 100.00
Note: Values in bold are above inertia for each dimension. TM, typical man; TW, typical woman.
534 Eur J Pain 18 (2014) 530–539
© 2013 European Pain Federation - EFIC®
S.F. Bernardes et al.
Is it a (fe)male pain?
Table 3 Cluster’s characteristics: Chi-squares on the frequency/percentage of participants’ sex, health-care training and personal pain experiences. Cluster 1
Participants’ sex Health-care training Personal chronic pain Past common pains Head Back Abdominals Musculoskeletal Urinary/Reproductive
Cluster 2
Cluster 3
Cluster 4 N
%
χ2
N
%
N
%
N
%
Man Woman Nurses Laypeople Yes No
9 20 14 15 10 19
31.0 69.0 48.3 51.7 34.5 65.5
18 41 36 23 11 48
30.5 69.5 61.0 39.0 18.6 81.4
7 17 15 9 10 14
29.2 70.8 62.5 37.5 41.7 58.3
3 8 3 8 3 8
27.3 72.7 27.3 72.7 27.3 72.7
0.068
Yes No Yes No Yes No Yes No Yes No
16 13 7 22 10 19 9 20 1 28
55.2 44.8 24.1 75.9 34.5 65.5 31.0 69.0 3.4 96.6
43 16 23 36 15 44 17 42 24 35
72.9 27.1 39.0 61.0 25.4 74.6 28.8 71.2 40.7 59.3
13 11 10 14 3 21 5 19 4 20
54.2 45.8 41.7 58.3 12.5 87.5 20.8 79.2 16.7 83.3
2 9 0 11 0 11 1 10 1 10
18.2 81.8 0.0 100.0 0.0 100.0 9.1 90.9 9.1 90.9
12.732*
5.357 5.428
8.268 7.183 2.591 17.557**
*Borderline significance (p = 0.005). **p = 0.001; values in bold are significantly different than expected if responses were random.
tioned pain associated with the urinary/reproductive system and, to a much lesser extent, musculoskeletal pain. Contrary to what was found for the typical man, two aetiology subcategories reached a moderate/high consensus, namely labour/puerperium and hormonal cycles, respectively. Like for the typical man, almost all participants reported pains of physical nature and, to a much lesser extent, psychological pain. Chi-square analyses (see ‘Data analyses’ section) showed no significant effects of health-care training or the participants’ sex on the proportion of common pains reported for the typical man and woman, respectively (p > 0.001). Two relevant dimensions were identified in the MCA, accounting for 22.16% and 13.67% of the total variance, respectively. Table 2 shows the discrimination measures of each variable for the two dimensions (the closer to 1, the better the value). For each dimension, only values above inertia (variance mean value) were considered, which are set in boldface in Table 2. Fig. 1 presents the topological configuration of the gendered patterns of commons pains (in lined squares). For clarity purposes, only the ‘mentioned’ (vs. ‘not mentioned’) answer categories are visible. As can be seen, dimension 1 opposes pains of a psychological versus physical nature, regardless of the targets’ sex – typical man (TM) or typical woman (TW), whereas dimension 2 differentiates between representations of two patterns of common physical pains, mainly associated with the typical woman. © 2013 European Pain Federation - EFIC®
The combined analysis of the two dimensions allowed us to identify four patterns of common pains (Fig. 1, lined squares). At the centre, there is a pattern of common pains more frequently and consensually associated with the typical woman (headaches) and typical man (back and musculoskeletal pains), respectively. The remaining three patterns of common pains are more specific and less consensual. In the upperright quadrant, there is a pattern of more specific common pains associated with the typical woman, namely abdominal, back and musculoskeletal pains. The lower-right quadrant shows another more specific pattern of common pains again mainly associated with the typical woman, namely pains due hormonal cycles, labour/puerperium and from the urinary/ reproductive system. Finally, the lower-left quadrant shows a pattern of common pains of psychological nature both for the typical woman and man. Finally, the results of the HCA validated the MCA solution and identified four clusters of individuals, closely matching the four patterns of common pains, respectively (Fig. 1, dashed squares). Cluster 2 included almost half of the participants, while clusters 1 and 3 included around a quarter/fifth of the participants, respectively. Cluster 4 only included a minority of participants. It should be noted that people who endorsed the most stereotypical pattern of common pains (cluster 2) also frequently referred to typical woman’s pains due to hormonal cycle and from the urinary/reproductive system. Table 3 characterizes Eur J Pain 18 (2014) 530–539
535
Is it a (fe)male pain?
each of the four clusters in terms of the frequency/ proportion of participants’ sex, health-care training and personal pain experiences. Chi-square analyses showed no significant differences between the four clusters in terms of health-care training or participant sex (p > 0.001). An analysis of variance also showed no age-related differences between the four clusters (M = 34.29, 35.10, 33.25 and 29.91, respectively): F (3,118) = 0.63; p > 0.05.
3.2 Personal past pain experiences and gendered patterns of commons pains The final aim of this study was to explore the association between personal past pain experiences and the endorsed gendered patterns of commons pains. Table 1 shows that, concerning men’s self-reports, the most mentioned pain regions were, by decreasing order of proportion, head, teeth, abdominals and, finally, back. Also, the most mentioned pain experiences were physical and musculoskeletal. Regarding women’s self-reports, the majority reported having headaches, followed by pain in the back, abdominals and teeth. Also, female participants reported pains mostly related to the urinary/reproductive system, caused by the hormonal cycles. Musculoskeletal pains were also reported by nearly a quarter of the subsample. Chi-square analyses only showed significant sex-related differences in self-reported pains from the urinary/reproductive system: χ2(1) = 10.34; p = 0.001. More importantly, we tested the association between the clusters and personal experiences of CP and common pains (see Table 3). Chi-square analyses revealed that the only significant difference between the clusters was found for personal experiences of pains from the urinary/reproductive system; while participants in cluster 2 reported more pain than expected, participants in cluster 1 reported less pain than expected. It should, however, be noted that a borderline significant result for personal headache experiences was also found, where participants in cluster 2 tended to report more headaches than expected.
4. Discussion The first goal of this study was to explore, among Portuguese laypeople and nurses, patterns of common pains more strongly associated with the typical man or woman. Generally, our results showed the presence of different gendered patterns of common pains. Back and musculoskeletal pains were largely and consensually associated with the typical man. Due to 536 Eur J Pain 18 (2014) 530–539
S.F. Bernardes et al.
methodological differences, a direct comparison of our results with those of Robinson et al. (2003b, 2004) seems unwarranted. However, our results may be indirectly related to these authors’ finding that injury was the type of pain event most associated with the typical man, given that injuries are most often associated with musculoskeletal pain. Moreover, and although a very low proportion of our participants mentioned pain aetiology for the typical man, it should be noted that effort and trauma/injury were still the two most mentioned subcategories. As for the typical woman, our results suggested the presence of more differentiated patterns of common pains. By far, the strongest and most consensual association was the headache. Then, two less consensual and more differentiated patterns of common pains emerged. First, consistent with Robinson et al. (2003b, 2004), there was a pain pattern related to the specificities of women’s reproductive systems, including pains due to labour/puerperium and hormonal cycles. Also, a second more differentiated pattern was found, which included back and musculoskeletal pains along with abdominal pain. Finally, it should be noted that the pattern including pain of psychological nature (e.g. emotional suffering) was equally associated with the typical man and woman. This result seems at odds with findings that have suggested that the female stereotype is more strongly associated with distress and somatization (e.g., Goudsmit, 1994; Hoffman and Tarzian, 2001). Although differences in methodological strategies may underlie such discrepancies, the fact that only around 9% of our participants mentioned pain of a psychological nature makes this finding unrepresentative, increasing the risk of being over interpreted. In summary, our data show that the patterns of common pains associated with the typical man were less specific and differentiated than the patterns associated with the typical woman. In fact, the only pattern associated with the typical man, which included back and musculoskeletal pain, was also (although to a lesser extent) associated with the typical woman, while there were also two other very specific pain patterns associated with the typical woman. Also, pain aetiology subcategories were more consensually associated with the typical woman than the typical man and their meanings were entirely different; as with the previous findings (e.g., Robinson et al., 2003b, 2004), internal causes (mostly related to the reproductive system) were more associated with the typical woman’s pains and external causes (effort, injury, trauma) were more frequently mentioned for the typical man’s pains. This suggests that, as other © 2013 European Pain Federation - EFIC®
S.F. Bernardes et al.
authors have noted (e.g., Bendelow, 2000; Grace and MacBride-Stewart, 2007), pain is more often perceived as part of the typical woman’s ‘normal’ body functioning, which may partially be accounted for by the intrinsic association of the female stereotype with hormonal and reproductive functions. At the same time, however, pain is perceived as a ‘foreign intruder’ in the typical man’s body. It should also be stressed that there is some overlap between these gendered representations of common pains and epidemiological data on sex-related differences in pain; women report feeling more pain throughout their lives than men (e.g., Holdcroft and Berkley, 2005; LeResche, 2000); head and abdominal pain (even excluding menstrual cramps) are clearly more prevalent among women (e.g. Berkley and Holdcroft, 1999; LeResche, 1999), and although back pain is one of the most prevalent pain conditions worldwide, it is also a type of pain where sex-related differences are not clear or consistent (e.g. LeResche, 1999, 2000). Also, a study by Stutts et al. (2009) has shown that male undergraduates reported more externally inflicted pains (e.g., broken nose, concussion) and female undergraduates reported more internal pains (e.g., head and abdominal). Therefore, and in line with other findings in psychological research, these gender representations (of common pain events) seem, on average, relatively accurate (Eagly and Dielman, 1997; Wood and Eagly, 2010). Moreover, and in line with the findings of Robinson et al. 2003b, 2004), such gendered representations of common pains were equally held by male and female participants. We agree with Robinson et al. (2003b) that this may reflect very consistent and homogeneous gender learning experiences. We also believe that our experimental task may not be strong enough to activate motivational factors that may account for sexrelated differences in the endorsement of gender representations (e.g., in-group bias, in order to maintain a positive social identity). In other words, associating types of pain with the typical man or woman does not seem as threatening to an individual’s gender identity than, e.g., associating personality traits (e.g., fragile, dependent, aggressive). The remaining goals of this study were to explore whether health-care training or personal past pain experiences were associated with the gendered patterns of common pains. With regard to health-care training, our findings showed that these gendered representations were equally shared by laypeople and nurses. This suggests that the presence/absence of training in nursing has no significant influence on what representations are endorsed or on their accu© 2013 European Pain Federation - EFIC®
Is it a (fe)male pain?
racy. This result may possibly be accounted for by the study’s focus on everyday common pains instead of clinical pain disorders. It also suggests that people’s numerous everyday observations of men’s and women’s pain experiences seem enough to allow for the development of relatively accurate gendered patterns of common pains, on average. As for the effects of personal pain experiences, our findings highlight a few associations between these and the inclusion of such pains in the endorsed representations. Specifically, participants from cluster 2, who more consensually endorsed the association of pains from the urinary/reproductive system and headaches to the typical woman, were the ones who also significantly reported more personal pains from the urinary/reproductive system and tended to report more headaches than expected. The reason why only these types of pains were associated with the endorsed representations of common pains is unclear. Moreover, the fact that no other personal pain experiences (including CP) showed a significant effect makes our findings far from being enough to support a general contention of an association between personal past pain experiences and the endorsed gendered patterns of common pains. We believe this issue should be further explored. Some shortcomings of this study may be pointed out. Although, compared with the samples of Robinson et al. (2003b, 2004), our participants were more heterogeneous in terms of age and educational background, the generalization of our findings to other populations with fewer years of education, other types of health-care training (e.g., doctors), cultural backgrounds or more pervasive and disabling pain experiences should be considered with caution. Despite these limitations, implications of our findings and future directions for research should be highlighted. In spite of their accuracy at a group level, such gendered representations may account for biases in the assessment and treatment of an individual’s pain experience. First, at a general level, the fact that pain is perceived as a ‘natural’ part of the typical woman’s body functioning may, as other authors have suggested (Bendelow, 1993, 2000), be associated with the expectation that women are better able to cope with pain, which, consequently, may account for the fact that women’s pain is more often under-valued and under-treated as compared to men’s pain (e.g., Hoffman and Tarzian, 2001). Second, at a more specific level, these representations may slant people’s perceptions of a specific (gendered) pain experience, depending on the sufferer’s sex. For example, if a headache is more associated Eur J Pain 18 (2014) 530–539
537
Is it a (fe)male pain?
with the female stereotype, will it be assessed and treated the same if it is being reported by a man or a woman? Paulson et al. (1999, 2002) report qualitative data on the unwillingness of doctors to diagnose males with fibromyalgia, which indirectly supports this contention. However, to the best of our knowledge, no authors have directly tried to test it. Third, the possibility that reporting a gendered pain experience may have an impact on how others perceive the sufferer’s gender identity should also be considered. For example, as compared with the typical man, will a man with migraines be perceived as equally masculine? One of our previous studies (Bernardes and Lima, 2010) showed that a man with chronic low-back pain was perceived as less typically masculine and more typically feminine and a woman with chronic low back pain was perceived as less typically feminine and more typically masculine. Given that this pattern of results was found with a more gender-neutral type of pain, it would be interesting to further explore the influence of more gendered common pains on men’s and women’s perceived gender identities. Finally, if living with a counter-stereotypical type of pain (e.g., a man with migraines) may influence how others perceive the sufferer’s gender identities, will it have an impact on the sufferer’s (phenomenological) pain experiences? For example, are men with migraines less willing to report their pain than men with traumatic pains? Paulson et al. (1999, 2002) highlighted the deep shame that some men felt when they were diagnosed with fibromyalgia. Also, Stutts et al. (2009) showed that men rated the intensity of pain events like a broken finger nail or hair pulled as higher than women, but women rated traumatic pains (e.g., concussion, burns and dislocated joints) as higher than men. Together, these findings seem to suggest that experiencing counter-stereotypical pains may influence the severity and emotional tone of pain experiences. In conclusion, a major contribution of this study, derived from the use of multivariate statistical analyses, was to highlight the complexity and multifaceted nature of gendered patterns of common pains. In doing so, it also raises important questions regarding the implications of such gendered representations for men’s and women’s pain experiences and how these are interpreted by others. Authors contributions S.F.B. took the responsibility for the integrity of the work as a whole, from its conception and design, analysis and inter-
538 Eur J Pain 18 (2014) 530–539
S.F. Bernardes et al.
pretation of data to the drafting, and final approval of the manuscript. S.A.S. contributed to the qualitative and quantitative data analyses and interpretation, wrote parts of the methods and results sections, and critically revised the entire manuscript. H.C. was responsible for the multivariate analyses, the figures and contributed to the critical revision of the manuscript. M.C. contributed to the conception and design of the study and was responsible for the data collection and content analysis. Finally, S.P. also contributed to the content analysis and wrote parts of the Methods section.
References Alabas, O., Tashani, O., Johnson, M. (2012). Gender role expectations of pain mediate sex differences in cold pain responses in healthy Libyans. Eur J Pain 16, 300–311. Amâncio, L. (1994). Masculino e Feminino: A Construção Social da Diferença (Porto: Edições Afrontamento). Augoustinos, M., Ahrens, C. (1994). Stereotypes and prejudice: The Australian experience. Br J Soc Psychol 33, 125–141. Bendelow, G. (1993). Pain perceptions, emotions and gender. Soc Health Illn 15, 273–294. Bendelow, G. (2000). Pain and Gender (Harlow: Prentice Hall/Pearson Education). Berkley, K., Holdcroft, A. (1999). Sex and gender differences in pain. In Textbook of Pain, 4th edn., P. Wall, R. Melzack, eds. (London: Churchill Livingstone) pp. 951–965. Bernardes, S.F., Lima, M.L. (2010). Being less of a man or less of a woman: Perceptions of chronic pain patients’ gender identities. Eur J Pain 14, 194–199. Carvalho, H. (2008). Análise de Multivariada de Dados Qualitativos: Utilização da Análise de Correspondências (SPSS) (Lisbon: Sílabo). Defrin, R., Eli, I., Pud, D. (2011). Interactions among sex, ethnicity, religion and gender role expectations of pain. Gend Med 8, 172–183. Dannecker, E., George, S., Robinson, M. (2007). Influence and stability of pain scale anchors for an investigation of cold pressor pain tolerance. J Pain 8, 476–482. Eagly, A.H., Dielman, A.B. (1997). The accuracy of gender stereotypes: A dilemma for feminism. Int Rev Soc Psychol 10(2), 11–30. Flick, U. (2007). Designing Qualitative Research: The SAGE Qualitative Research Kit (London: Sage Publications). Goudsmit, E. (1994). All in her mind! Stereotypic views and the psychologisation of women’s illness. In Women and Health: Feminist Perspectives, S. Wilkinson, C. Kitzinger, eds. (London: Taylor & Francis) pp. 7–12. Grace, V., MacBride-Stewart, S. (2007). Women get this: Gendered meanings of chronic pelvic pain. Health (London) 11, 47–67. Greenacre, M. (2007). Correspondence Analysis in Practice, 2nd edn (London: Chapman & Hall / CRC). Hair, J., Black, W., Babin, B., Anderson, R. (2010). Cluster analysis. In Multivariate Data Analysis: A Global Perspective, 7th edn. (Upper Saddle River: Pearson Education) pp. 477–536. Hayes, A., Krippendorff, K. (2007). Answering the call for a standard reliability measure for coding data. Commun Methods Meas 1, 77–89. Hoffman, D., Tarzian, A. (2001). The girl who cried pain: A bias against women in the treatment of pain. J Law Med Ethics 29, 13–27. Holdcroft, A., Berkley, K. (2005). Sex and gender differences in pain and its relief. In Wall and Melzack’s Textbook of Pain, 5th edn S. McMahon, M. Koltzenburg, P. Wall, R. Melzack, eds. (Edinburgh: Elsevier Churchill Livingstone) pp. 1181–1197. Keogh, E., Denford, S. (2009). Sex differences in perceptions of pain coping strategy usage. Eur J Pain 13, 629–634. Krueger, J. (1996). Personal beliefs and cultural stereotypes about racial characteristics. J Pers Soc Psychol 71, 536–548. LeResche, L. (1999). Gender considerations in the epidemiology of chronic pain. In Epidemiology of Pain, I.K. Crombie, P.R. Croft, S.J. Linton, L. LeResche, M. Von Korff, eds. (Seattle: IASP Press) pp. 43–52.
© 2013 European Pain Federation - EFIC®
S.F. Bernardes et al.
LeResche, L. (2000). Epidemiologic perspectives on sex differences in pain. In Sex, Gender and Pain, R. Fillingim, ed. (Seattle: IASP Press) pp. 233–249. Merskey, H., Bogduk, N., eds. (1994). Classification of the Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms, 2nd edn (Seattle: IASP Press). Mooi, E., Sarstedt, M. (2011). Cluster analysis. In A Concise Guide to Market Research. The Process, Data and Methods Using IBM SPSS Statistics. (Berlin: Springer-Verlag) pp. 237–284. Muhr, T. (2004). Atlas.Ti V5.0, the Knowledge Workbench: User’s Guide and Reference, 2nd edn (Berlin: Scientific Software Development). Paulson, M., Danielson, E., Norberg, A. (1999). Nurses’ and physicians’ narratives about long-term non-malignant pain among men. J Adv Nurs 30, 1097–1105. Paulson, M., Danielson, E., Soderberg, S. (2002). Struggling for a tolerable existence: The meaning of men’s lived experiences of living with pain with fibromyalgia type. Qual Health Res 12, 238–249. Pimenta, C., Teixeira, M. (1996). Questionário de dor McGill: Proposta de adaptação para a língua portuguesa. Revista da Escola de Enfermagem da USP 30, 473–483. Ramos, M., Carvalho, H. (2011). Perceptions of quantitative methods in higher education: Mapping students profile. High Educ 61, 629–647. Robinson, M.E., Gagnon, C., Dannecker, E., Brown, J., Jump, R., Price, D. (2003b). Sex differences in common pain events: Expectations and anchors. J Pain 1, 40–45.
© 2013 European Pain Federation - EFIC®
Is it a (fe)male pain?
Robinson, M.E., Gagnon, C., Riley, III J., Price, D. (2003a). Altering gender role expectations: Effects on pain tolerance, pain threshold and pain ratings. J Pain 4, 284–288. Robinson, M.E., George, S., Dannecker, E., Jump, R., Hirsh, A., Gagnon, C., Brown, J. (2004). Sex differences in pain anchors revisited: Further investigation of ‘most intense’ and common pain events. Eur J Pain 8, 299–305. Robinson, M.E., Riley, III, J., Myers, C., Papas, R., Wise, E., Waxenberg, L., Fillingim, R. (2001). Gender role expectations of pain: Relationship to sex differences in pain. J Pain 2, 251–257. Robinson, M.E., Wise, E. (2003). Gender bias in the observation of experimental pain. Pain 104, 259–264. Robinson, M.E., Wise, E. (2004). Prior pain experience: Influence on the observation of experimental pain in men and women. J Pain 5, 264– 269. Saldaña, J. (2009). The Coding Manual for Qualitative Researchers (Los Angeles: Sage). Stutts, L., McCulloch, R., Chung, K., Robinson, M. (2009). Sex differences in prior pain experience. J Pain 12, 1226–1230. Wood, W., Eagly, A. (2010). Gender. In Handbook of Social Psychology, 5th edn S. Fiske, D. Gilbert, G. Lindzey, eds. (Hoboken, NJ: John Wiley & Sons) pp. 629–667.
Eur J Pain 18 (2014) 530–539
539