Republic of Iraq Kurdistan Regional Government Ministry of Higher Education & Scientific Research University of Sulaimani College of Pharmacy
COMPARISON OF ACUTE AND DELAYED ANTIEMETIC EFFECT AND THE CHANGE IN QUALITY OF LIFE BY (APREPITANT,ONDANSETRON AND DEXAMETHASON) AND (ONDANSETRON, DEXAMETHASON) IN HODGKINS LYMPHOMA PAYIENTS RECEIVING HIGHLY EMETOGENIC CHEMOTHERAPY IN HIWA HOSPITAL A Thesis submitted to the council of the college of Pharmacy at University of Sulaimani in Partial Fulfillment of the Requirements for the Degree of Master of Science in Pharmacy Practice-Hospital Setting
Dara Abdulla Mohammed
B.Sc. Pharmacy 2011-2012 Supervisor
Dr. May Taha Sdiq Assistant Professor-College of Pharmacy/University of Baghdad
Sulaimani 2016 A.D
1438 A.H
Kurdi2716
صدق هللا العظيم سورة المجادلة آيە ()11
Supervisor certification I certify that this thesis was carried out under my supervision by student Dara Abdulla Mohammed entitled (Comparison of acute and delayed antiemetic effect and the change in the quality of life by (Aprepitant,Odansetron and Dexamethason) and (Odansetron, Dexamethason) in Hodgkin's Lymphoma patients receiving highly emetogenic chemotherapy in Hiwa Hospital) and do herby recommend that it is accepted as a partial fulfillment of the requirement for degree of Master of Science in Pharmacy Practice-Hospital Setting
Signature Supervisor
Assistant Professor Dr.May Al-Sabbagh
EXAMINATION COMMITTEE CERTIFICATION We, the examining committee, certify that we have read this thesis entitled {Comparison of acute and delayed antiemetic effect and the change in the quality of life by (Aprepitant,Odansetron and Dexamethason) and (Odansetron, Dexamethason) in Hodgkin's Lymphoma patients receiving highly emetogenic chemotherapy in Hiwa Hospital} and have examined the candidate pharmacist Dara Abdulla Mohammed in its contents and it meets the standard requirements for the degree of Master of Science in Pharmacy Practice-Hospital Setting. Signature:
Signature:
Name: Dr. Mohammed Omer Mohammed
Name: Dr. May taha sdiq
Title: Professor
Title: Assistant Professor
Date: 24/12/2016
Date: 24/16/2016
( Chairman )
( Supervisor-Member )
Signature:
Signature:
Name: Dr. Hiwa Khdir saaed
Name: Dr.Niazi Burhanaldin Husamaldin
Title: Lecturer
Title: Lecturer
Date: 24/12/2016
Date: 24/12/2016
( Member )
( Member )
Approved by the Head of Clinical Pharmacy Department Signature: Name: Hiwa Khdir saaed Title: Lecturer Date: 24/12/2016
Dedication
To my father To my mother To my Wife To my brother & sister To my son & daughter
Acknowledgement Thanks for Great God for helping me to accomplish this work. I would like to express my deep gratitude and endless appreciation to my teacher and supervisor, Dr.MayAl-Sabbagh, for her continuous support, guidance, and encouragement through providing me valuable advice during the entire period of conducting this thesis. I am indebted to Dean of School of Pharmacy-Sulaimani University. Dr. Hiwa K. Saaed for his guidance and real support from beginning and throughout the study. I am very much thankful to my teacher Dr. Zheen Aorahman/ Head of Clinical Pharmacy department for his continuous help and guidance. My sincere appreciation to Dr. Najmaddin Khoshnaw, who provided me with valid notes and advice. Great thanks to Dr. Ahang Esmail Amin; who support me during my study. Also special thanks to Dr. Osama F. Al-Qaisi for his efforts in statistical analysis.
Finally, I shouldn’t forget all my colleagues
Pharmacy College who helped and supported me during the study.
contents Subject
Page no.
List of contents
I
List of tables
II
List of graphs
III
List of abbreviations
IV
Abstract
V
Chapter one Introduction
2
General objectives
6
Literatures review
7
1.1. Background
7
1.2. Definitions of nausea, vomiting and retching
9
1.3. Chemotherapy- induced nausea and vomiting
10
1.4. Mechanisms of CINV
11
1.5. Incidence and Impact CINV
13
1.6. Classification
15
1.7. Risk Factors
17
1.8. Prophylaxis and treatment options
18
1.9. Chemotherapy drug emetogenicity
21
1.10. Poor control of emesis
50
1.11. Cannabinoids and medical marijuana
51
1.12. Complementary therapies
53
Chapter two Patients & Methods
57
2.1. Study design & settings
57
2.2. Population of the study
57
2.3. Medication
57
2.4. Sampling & randomization
58 I
2.5. Treatment protocol
59
2.6. Assessment
61
2.7. Ethical protocol
62
Chapter three Results
65
Chapter four Discussion
81
Chapter five Conclusions & Recommendations
91
References
93
II
List of tables Title
Page no.
Table 1.1: Classification of the emetogenic potential antineoplastic agents. Table 1.2: Roles of 5HT and substance P in CINV. Table 1.3: Agents used for prophylaxis and treatment of CINV.
of
Table 2.1: Treatment protocol Table 3.1: Demographic characteristics of study participants. Table 3.2: Nausea scores and emetic effect of study participants. Table 3.3: Vomiting scores and emetic effect of study participants. Table 3.4: Distribution of demographic characteristics and rescue medications of study participants according to study groups. Table 3.5: Distribution of nausea scores and emetic effect of study participants according to study groups. Table 3.6: Distribution of vomiting scores and emetic effect of study participants according to study groups. Table 3.7: Distribution of nausea scores of study participants according to study groups. Table 3.8: Distribution of vomiting scores of study participants according to study groups. Table 3.9: Distribution of nausea and vomiting scores of treatment group according to administration days. Table 3.10: Distribution of total nausea and vomiting scores of study participants aging less than 40 years according to study groups. Table 3.11: Distribution of total nausea and vomiting scores of study participants aging 40 years and more according to study groups. Table 3.12: Distribution of total nausea and vomiting scores of male study participants according to study groups. Table 3.13: Distribution of total nausea and vomiting scores of female study participants according to study groups.
III
16 18 20 61 65 67 68 70 72 73 74 75 76 77
78
78 79
List of figures Subtitle
Page no.
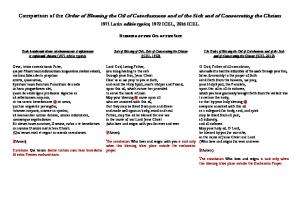
Figure 1.1: The main inputs into the vomiting center that lead to the vomiting.
13
Figure 2.1: Sampling and randomization schedule
62
Figure 3.1: Age distribution of study participants.
66
Figure 3.2: Gender distribution of study participants.
66
Figure 3.3: Total emesis effect of all study patients.
69
Figure 3.4: Distribution of rescue medications.
69
Figure
medications
71
Figure 3.6: Distribution of nausea score emesis effect
72
3.5:
Distribution
of
rescue
according to study groups.
according to study groups. Figure 3.7: Distribution of vomiting score emesis effect
74
according to study groups. Figure 3.8: Distribution of nausea scores according to
75
study groups. Figure 3.9: Distribution of vomiting scores according to
76
study groups. Figure 3.10: Distribution of total nausea and vomiting scores according to days of administration.
IV
77
List of abbreviations Abbreviations 5-HT3 AC ANV APR ASCO CINV DNA FDA FILE HEC IV LEC MASCC/ESMO
Meanings Serotonin receptor The Doxorubicin plus Cyclophosphamide Anticipatory Nausea and Vomiting Aprepitant American Society of Clinical Oncology Chemotherapy-Induced Nausea and Vomiting Deoxyribo Nucleic Acid US Food and Drug Administration Functional living index- Emesis Highly Emetogenic Chemotherapy Intravenous Low Emetogenic Chemotherapy Multinational Association of Supportive Care in
MEC
Cancer/Economic Society for Medical Oncology Moderately EmetogenicChemotherapy
MinEC NCCN NIDL NEPA NK-1 NK1R QoL RNA RR SD SPSS UK USA WHO
Minimal EmetogenicChemotherapy National Comprehensive Cancer Network No effect on daily life NetupitantPlus Palonosetron Neurokinin-1 NK1 Receptor Quality of Life Ribo Nucleic Acid Risk Ratio Standard Deviation Statistical Package for Social Sciences United Kingdom United States of America World Health Organization V
Abstract Introduction: Chemotherapy-induced nausea and vomiting will be around as long as cytotoxic chemotherapy is used to treat cancer. Nausea and vomiting are common and feared symptoms among cancer patients, and up to 80% of patients will
experience
chemotherapy-induced
nausea
and
vomiting
without
prophylactic therapy. Aim of Study: To compare the acute and delayed antiemetic effect and the change in the quality of life by (Aprepitant, Ondansitron and Dexamethason) and (Ondansitron, Dexamethason) in Hodgkin's Lymphoma patients receiving highly emetogenic chemotherapy in Hiwa Hospital Patients & Methods: A randomized single blind controlled clinical trial conducted in Hiwa Teaching Hospital in Sulaimani city for period from 1st of January to the end of December, 2015 on convenient sample of 70 Hodgkin's lymphoma patients. Patients received either the treatment (Aprepitant, Ondansitron and Dexamethason) or the standard regimen (Ondansitron, Dexamethason) in a 1:1 ratio according to a computer-generated, random allocation schedule. Results: There was no significant difference between two study groups in mean nausea scores at first day (p=0.3). A significant higher mean nausea and vomiting anti-effect scores was observed for treatment groups patients at 2nd , 3rd and 4th days than standard group patients (p<0.05). There was a significant higher total mean nausea and vomiting anti-effect scores for treatment group patients (p=0.001). Conclusions: The use of Aprepitant, Ondansitron and Dexamethason regimen showed superior and valuable results in prevention of cancer induced nausea and vomiting by patients on chemotherapy V
Chapter One Literatures review
Introduction
Introduction World Health Organization (WHO) defined cancer as a chronic health problem like hypertension and diabetes that increasing rapidly in incidence all over the world. It is predicted to be a worldwide critical cause of morbidity and mortality in the next few decades. By year 2020 in the world approximately 24.6 million of people will live with cancer with about 12.5% of all deaths attributable to cancer1. Cancer is a class of disease in which group of cells show out of control growth, invasions and sometime metastasis to different parts of the body2. Chemotherapeutic agents are the preference drug typically cytotoxic in nature, which can destroy most of cancer cells. Chemotherapy works by preventing or slowing the increase of cancer cells which developand divide quickly3. Nausea and vomiting are among the most distressing and debilitating adverse effects identified by patients receiving chemotherapy treatment4. Cytotoxic chemotherapies used in the treatment of different malignancies are known to cause significant side effects. One of the immediate side effects that are most distressing to the patients is nausea and vomiting. Poorly controlled chemotherapy-induced nausea and vomiting (CINV) can lead to dehydration, malnutrition and electrolyte imbalance and can cause physical damage, including Mallory-Weiss tears of the esophagus. These- symptoms can result in treatment delays, or a patient may refuse to continue treatment. CINV can also have an economic impact on the management of patients with cancer, including increased hospitalization and nursing costs 5. Chemotherapy Induced Nausea and Vomiting will be around as long as cytotoxic chemotherapy is used to treat cancer 6. Nausea and vomiting are common and feared symptoms among cancer patients, and up to 80% of patients will experience CINV without prophylactic therapy 7.
2
Introduction Chemotherapy Induced Nausea and Vomiting is also a frequent cause of patient non-adherence to chemotherapy, which may impact control of cancer and survival of patients 8.In the past three decades, more effective antiemetic medications were introduced and widely adopted. Serotonin (5-HT3) receptor antagonists are considered safe and work alone or in combination with corticosteroids (eg, dexamethason) or other agents. Most recently, neurokinin-1 (NK-1) receptor antagonists, a new class of antiemetic, have been studied. One such drug (aprepitant [Emend]) has been approved for use in combination with other antiemetic9. CINV can be described as acute, delayed and anticipatory according to time course. The acute form of CINV is the well-recognized form. It is also known as post-treatment CINV. Acute CINV is usually defined as nausea and/or vomiting within the first 24 h after administration of chemotherapy. Delayed CINV is usually defined as nausea and/or vomiting that begins after the first 24 h of administration of chemotherapy. Delayed CINV may last for as long as 120 h after chemotherapy administration. Anticipatory CINV occurs before the second or later course of chemotherapy. Anticipatory CINV is a learned or conditioned response to poorly managed CINV during previous courses of chemotherapy. As a learned response, anticipatory CINV has a strong psychological component and does not respond well to antiemetic prophylaxis or treatment8, 9. However, it has been shown to respond to behavioral interventions. The most effective approach to preventing anticipatory CINV is to prevent nausea and vomiting associated with the patient’s earlier courses of chemotherapy
10, 11
.
Risk factors for CINV fall into patient-related, disease related and treatmentrelated categories. Patient-related risk factors include age younger than 50 years, female sex, poor performance status, history of light alcohol use (heavier drinkers have less emesis), a prior history of nausea and/or vomiting associated with pregnancy or motion sickness, increased anxiety, a history of CINV with prior exposure to 3
Introduction Chemotherapy, and low social functioning
10, 12
. Disease-related features such
as the primary site of the cancer, the histological subtype, clinical stage, and presence of end organ dysfunction may further impact the probability of emesis. The intrinsic risk of the chemotherapy regimen is the main risk factor for the overall degree of CINV and can vary depending on the class of drug, dose, schedule, and route of administration used. The current classification of the risk of emesis is mostly based on the intrinsic emetogenic potential of the chemotherapy regimen
12
, which is stratified as follows: high emetogenic
potential (>90% risk of inducing vomiting after chemotherapy administration), moderate emetogenic potential (>30–90% risk), low emetogenic potential (10– 30% risk), and minimal emetogenic potential (<10% risk) 13. More than 90% of patients undergoing highly emetogenic chemotherapy (HEC) will experience emesis without antiemetic prophylaxis, and 30% to 90% of those undergoing moderately emetogenic chemotherapy (MEC) will vomit without the prophylactic administration of antiemetics. From 10% to 30% of the patients receiving low emetogenic chemotherapy (LEC), and <10% of patients receiving minimal emetogenic chemotherapy (MinEC), will experience emesis without the administration of antiemetics8 .The dose, frequency, and length of administration, as well as the combination of agents may impact the emetogenicity of the chemotherapy14, 15. Poorly controlled CINV may lead to nutrient depletion, reduced functional ability, diminished quality of life, or the premature discontinuation of chemotherapy. The use of prophylactic antiemetic medications in patients undergoing HEC may reduce the incidence of CINV to as low as 30%
15
.A
multidrug regimen containing a 5-hydroxytryptamine receptor antagonist (5HT3RA) is the standard approach for CINV prophylaxis. Drugs in this category include dolasetronmesylate, granisetron, ondansetron, palonosetron, and tropisetron, with palonosetron recommended as the preferred 5-HT7 RA 4
Introduction for CINV prophylaxis with MEC by the guidelines of the National Comprehensive Cancer Network (NCCN), the Multinational Association of Supportive Care in Cancer/Economic Society for Medical Oncology (MASCC/ESMO), and the American Society of Clinical Oncology (ASCO)15, 18
.
Aprepitant (APR) is a selective NK-1 antagonist for the substance P in the central nervous system. Several eligible clinical trials evaluating the antiemetic effect of APR in patients receiving high doses of cisplatin (≥70 mg /m2) or anthracycline/cyclophosphamide demonstrated that APR combined with the standard antiemetic medication, comprising 5-HT3 antagonistand DEX, significantly improved complete response (no emesis and no rescue treatment) compared to the standard antiemetic therapy 19. APR is shown to be effective against acute as well as delayed emesis, in which the efficacy is independent of gender 20
Rationale of study 1. High rates of chemotherapy induced-nausea and vomiting cases in Hiwa Hospital and help cancer patients. 2. Selection of appropriate antiemetic agents to decrease CINV. 3. Lowering health and economic burden caused by CINV. 4. Encouraging further researches on this subject.
5
Introduction General objectives To compare the acute and delayed antiemetic effect and the change in the quality of life by (Aprepitant, Ondansitron and Dexamethason) and (Ondansitron, Dexamethason) in Hodgkin's Lymphoma patients receiving highly emetogenic chemotherapy in HiwaHospital.
6
Introduction
Literatures review 1.1. Background Cancer is a group of more than 200 different diseases, and can generally be described as an uncontrolled growth and spread of cells, in which abnormal cells are able to invade other tissues through the lymphatic system or the bloodstream
21
.The incidence of cancer is rising, and it is estimated that by
2020, globally, more than 15 million people will experience cancer. The main goal of a cancer treatment program is to cure or considerably prolong the life of patients, and to ensure the best possible quality of life to cancer survivors 21. It may be caused by internal factors (such as inherited mutation, hormones, immune deficiencies, conditions and mutations arising from metabolism) or external factors (tobacco, radiation, chemicals or infectious organisms) 22. The general strategies for cancer treatment include surgery, radiotherapy, and chemotherapy, or combined strategies of these. These are supplemented by more specialized therapies, such as immunotherapy or hormone therapy, which can be applied only to some types of cancer. Transplantation involving stem cells, or bone marrow, is another method of treatment, which is usually used in hematologic malignancies23. The oldest cancer treatment is surgery. It provides the greatest chance of cure, and is generally used for solid tumors; particularly those which have not yet metastasized to other parts of the body. Radiotherapy involves the use of highenergy particle beams or waves (radiation), such as X-rays, gamma rays, or neutrons, for treating cancer. The radioactive material transfers its energy into highly energetic electrons which ionize the matter they hit, such as water and/or proteins or other molecules of the cell cytoplasm, or Ribo Nucleic Acid (RNA) 7
Introduction and Deoxyribo Nucleic Acid (DNA). This ionization alters the molecules and this leads to cell death, or inhibits cell division. Although radiation is more harmful to cancerous cells than normal cells, one of the major weaknesses of radiotherapy is that it is impossible to treat only cancerous cells, without affecting the surrounding healthy cells 24. Chemotherapy uses chemical agents in the treatment of cancer, and is particularly appropriate for cancers that have metastasized and cannot be treated any longer by localized methods such as surgery and radiation. Chemotherapy has long been one of the most important parts of cancer treatment. The main goals of chemotherapy vary, and can range from intentionto-cure to provision of comfort (i.e. palliation) 25. Chemotherapeutic agents can be administered intravenously, orally, in cycles, often over a number of months. In the broad sense, chemotherapeutical agents act by creating toxic effects on dividing cells (i.e. altering the synthesis and function of DNA and impairing mitosis), effectively targeting fast-dividing cells. However, this frequently results in severe damage to normal tissues, leading to side effects such as bone marrow suppression, and increased susceptibility to infection, nephrotoxicity, anorexia, alopecia, diarrhea, nausea and vomiting. The optimum goal is to find a treatment modality that specifically kills malignant cells while causing few or no side effects26. Major advances in different cancer treatment modalities (i.e. surgery, chemotherapy, radiotherapy, hormonal therapy, and biological response modifiers) have been made, and people are now living longer with cancer than they were in the past. However, cancer patients suffer from a range of physical, physiological, and psychological symptoms during their cancer journey. These symptoms are either directly related to the adverse effects of cancer, or arise from the different types of treatments, and may range from mild and temporary to severe, chronic, and life threatening 27.
8
Introduction The quality of life (QoL) and degree of suffering of patients with cancer is determined by the presence and intensity of these symptoms. Symptom prevalence and management are crucial in the clinical setting, because they enable health-care professionals to focus on the most prevalent symptoms, anticipate potential problems, and plan the type of care and symptom management accordingly 27. 1.2. Definitions of nausea, vomiting and retching 1.2.1. Nausea The word “nausea” originally referred to seasickness, and is derived from theGreek word “naus”, meaning ship
28
. Nausea is a separate but related
symptom to vomiting and retching. Nausea has been defined as “an unpleasant feeling of the need to vomit, often accompanied by autonomic sensations”
29
.
Others define nausea as “a subjective and unobservable phenomenon that may or may not culminate in vomiting”. It is synonymously described as feeling "sick to the stomach”. It is a disagreeable feeling experienced in the back of the throat, the epigastrium, and may be accompanied by pallor, cold clammy skin, increased salivation, faintness, tachycardia, and diarrhea. It is often associated with decreased gastric functioning, such as hypotonicity, hypoperistalsis, and hyposecretion30 1.2.2. Vomiting Vomiting is defined as “a forceful expulsion of the contents of the stomach, duodenum, or jejunum through the oral cavity”. Vomiting can be objectively quantified by frequency of occurrence and by the volume. Vomiting can be classified according to three phases: the first phase (pre- ejection or prodromal phase) is usually accompanied by nausea, and sometimes retching, as the gastrointestinal tract prepares itself for an emetic episode. Actual expulsion of stomach contents occurs in the second phase (ejection phase). The third phase is the post-ejection phase, when vomiting has stopped, nausea dissipated, and the person usually feels better 31. 9
Introduction 1.2.3. Retching “Retching is the attempt to vomit without bringing anything up”. It can be described by such terms as “gagging”, “dry heaves”, and “attempting to vomit without results”. Retching occurs with a rhythmic contraction of the diaphragm, the rectus abdominis, and the external intercostal muscles31. 1.3. Chemotherapy- induced nausea and vomiting CINV can be defined as nausea and vomiting that occurs in patients receiving chemotherapy. It can be classified according to three phases (acute, delayed and anticipatory) 32. 1.3.1. Acute CINV Acute CINV is typically defined as nausea and/or vomiting within the first 24 hours after chemotherapy administration. Vomiting, in the absence of effective antiemetic prophylaxis, most commonly begins within one to two hours of chemotherapy, and typically peaks in the first four to six hours. The actual period of acute nausea and vomiting is affected by many factors (including specific patient risk factors, which are explored in the following section), but are mainly influenced by the chemotherapy agent’s emetogenicity, and prescribed antiemetic drugs33. 1.3.2. Delayed CINV Delayed CINV is usually defined as nausea or vomiting that begins after the first 24 hours of chemotherapy administration. Although the duration of the delayed phase has not been fully defined, it may last for 5-7 days. Regardless of the regimen used, the frequency and the number of episodes of nausea and vomiting may be less in the delayed phase, compared with acute CINV. However, control and treatment of the delayed CINV, particularly delayed nausea, with current antiemetic medications is more difficult to manage than acute nausea and vomiting33.
10
Introduction 1.3.3. Anticipatory CINV Anticipatory nausea and vomiting (ANV) often occurs prior to the second or subsequent administration of chemotherapy. It occurs almost exclusively in patients who have experienced poorly controlled nausea and vomiting during previous courses of chemotherapy 34. Although several studies consider ANV as a conditioned response, it is not only a learned response and can occur without prior exposure to chemotherapy, depending on patients’ emotional distress and expectations 34, 35. 1.3.4. Breakthrough and refractory CINV Breakthrough and refractory CINV are two other terms that may be used with reference to chemotherapy. Breakthrough CINV can be defined as nausea and vomiting during any phase of the chemotherapy cycle, despite antiemetic prophylaxis. Breakthrough CINV is defined as nausea and vomiting that occurs despite standard preventative therapy (antiemetic prophylaxis), either in the acute or delayed phase. Refractory CINV is also described as a failure to respond to prevention and/or intervention during a previous cycle of treatment. For clinical purposes, if a patient vomits and/or retches twice, or experiences 4 hours of moderate to severe nausea, within 24 hours, it is considered significant breakthrough CINV, which requires intervention32.
1.4. Mechanisms of CINV In order to understand the approach to CINV and modern antiemetic treatment, it is crucial to obtain an understanding of the pathophysiology underpinning the emetic response. The pathophysiology of CINV is very complex, and not yet completely understood. This (the lack of understanding) might be related to different mechanisms being responsible for nausea and vomiting in the different phases. Furthermore, the mechanism within one chemotherapy agent may be different in another32.
11
Introduction 1.4.1. Summary of pathways by which chemotherapeutic agents mayproduce an emetic response Administering chemotherapy drugs is considered one of the stimuli of nausea and vomiting through effects at a number of sites. The mechanism that is best supported by research involves an effect on the upper small intestine (Figure 1)36. After the administration of chemotherapy, the Enterochromaffin cells (in the gut) are stimulated, leading to localizedexocytotic release of Serotonin (5hydroxytryptamine), which then interact with the chemoreceptor 5hydroxytryptamine 3, which are located on theVagus nerve in the wall of the intestine
31
. Subsequently, an impulse will be transmitted primarily to the
nucleus Tractussolitarius, and then the chemoreceptor trigger zone in the brain. Receptors (neurokinin-1, 5-HT3, and dopamine-2) are present in the dorsal vagal complex, and bind to neurotransmitters (substance P, 5HT and dopamine, respectively). Efferent fibers project from the dorsal vagal complex to the final effecter of the emetic reflex in the brain stem 31. Antineoplasic agents may also induce nausea and vomiting through interaction with the area postremawithin the dorsal vagal complex. Other potential sources of efferent include a number of structures in the temporal lobe, such as the amygdala36. Most anti-emetic medications, such as NK1 receptor antagonists, that are able to prevent or control many types of emesis (induced by drugs, motion, vagal stimulation, etc.) work by blocking afferent inputs (cerebral, vestibular, area postrema, and gut) for nausea and vomiting that converge on the nucleus of the solitary tract in the caudal hindbrain. The sensory pathways for nausea and vomiting are well understood (e.g. vagal and vestibular inputs); however, the critical problem of defining the convergent neural circuitry that generates nausea and vomiting is still largely unexplained. This might be one of the main reasons that make designing effective treatments to control nausea and vomiting complicated28. 12
Introduction
Figure 1: The main inputs into the vomiting center that lead to the vomiting36.
1.5. Incidence and Impact of CINV The overall incidence of CINV is challenging to estimate, as risks vary greatly depending on the emetogenicity of chemotherapy and a number of risk factors. Nevertheless, it is generally accepted that without appropriate prophylaxis, 70% to 80% of all cancer patients receiving chemotherapy experience nausea and/or vomiting
37
. Even with prophylaxis, observational studies indicate that
as many as half of patients may experience uncontrolled nausea or vomiting 38; for example, Grunberg et al reported that greater than 35% of patients experienced nausea within 24 hours of chemotherapy, with 54% experiencing nausea and 32% experiencing vomiting in the following 4 days 39. While improvements in antiemetic therapy have enabled improvements in quality of life for patients undergoing emetogenic chemotherapy, unmet needs 13
Introduction remain 40. The burden that uncontrolled CINV places on patients and their families and careers can be substantial, impacting both physical well-being and quality of life. The direct physiological effects of nausea and vomiting include metabolic imbalances (hypokalemia, hyponatremia, hypochloremic alkalosis), degeneration of functional ability and performance status, nutrient depletion, anorexia, and esophageal tears . Moreover, if the symptoms of severe emesis are not recognized and treated, a number of potentially serious complications could arise. These may include dehydration, weight loss, metabolic disorders, dental erosion, wound dehiscence, and aspiration pneumonia 41. Beyond its direct physiological effects, CINV can affect diverse aspects of patients’ quality of life, such as daily functioning, leisure activities, and the enjoyment of food and drink. Interestingly, there is some evidence to suggest that nausea often has a greater impact on quality of life than vomiting in patients receiving chemotherapy 42. Moreover, consideration should be given to the knock-on effects of CINV. Haiderali et al estimated the total costs associated with CINV at $779 per patient following the first chemotherapy cycle, with more severe CINV attracting higher costs 43. Perhaps more worrisome, severe CINV may lead to a clinical decision to delay, reduce, or even stop chemotherapy. Although continued chemotherapy can substantially improve life expectancy and quality of life, many patients fear that side effects will reduce their overall quality of life, particularly during the palliative care phase; discontinuation of chemotherapy may therefore be a particular challenge in the palliative stages of treatment44.
14
Introduction 1.6. Classification of CINV CINV is typically classified based on the timing (or phase) of the nausea and/or vomiting in relation to chemotherapy. Anticipatory nausea and vomiting occurs prior to administration, and is thought to be a conditioned response to a negative chemotherapy experience, occurring in up to 20% of patients by the fourth treatment cycle. Anticipatory nausea and vomiting is difficult to treat once developed
45
. Therefore, current guidelines emphasize the importance of
effectively preventing acute or delayed CINV (the negative experience) from the first time chemotherapy is administered, thereby avoiding the subsequent development of a conditioned response. However, if anticipatory nausea does occur, behavioral therapy with systematic desensitization is the primary treatment recommended 46. Acute CINV typically occurs within 24 hours after chemotherapy administration, while delayed CINV usually develops 24 to 120 hours after administration 47. Delayed CINV has a higher incidence than acute CINV and also has a pronounced impact on patient quality of life 44. Evidence suggests, however, that delayed CINV is underreported by patients, and its incidence is underestimated by most oncology physicians and nurses 39; while uncontrolled acute CINV is correlated with escalation of antiemetic treatment, the same cannot be said for delayed CINV 38. Chemotherapy agents and regimens are classified based on the risk of nausea and vomiting they carry. Such classification of emetogenicity provides a valuable framework for guiding antiemetic treatment decisions in practice 45. In the mid-1990s, Hesketh and colleagues developed a classification scheme in which individual chemotherapy agents were assigned to 1 of 5 emetogenic levels 36. An algorithm was then devised to determine the emetogenicity of multiple-agent regimens by identifying the most emetogenic agent in the combination and assessing the relative contribution of the other agents 36. More 15
Introduction recently, a 4-level classification for single antineoplastic agents has been agreed by the major expert bodies in cancer care, with new agents being added as they are developed (Table 1) 46. Low, moderate and high emetogenic risk chemotherapy are commonly abbreviated as LEC, MEC and HEC, respectively.
The above classifications are primarily applicable to single-day chemotherapy cycles. However, the assessment of emetogenicity has become complicated by the increasing use of multi-day chemotherapy regimens—in part triggered by a rise in the use of oral chemotherapy agents, which tend to be used in extended regimens. Antiemetic treatment decisions for multi-day regimens are complicated by the overlap of acute and delayed emesis after the first day of chemotherapy. In addition, some agents only become consistently emetogenic after a week or more of continuous administration 45. This area is relatively underrepresented in the literature and, crucially, the established emetogenicity scales have not been validated against multi-day regimens. A practical method 16
Introduction for assessing the emetogenic risk of multi-day regimens was proposed as part of a recent evaluation of multi-day antiemetic therapy. This study adopted an emetogenicity classification for 3- to 5-day chemotherapy regimens based on a modification of the Hesketh scale. Although not formally validated, this approach offers a pragmatic option for use in routine practice48. 1.7. Risk Factors Beyond the inherent emetogenic risk of each chemotherapy regimen, a number of factors affect the risk of CINV in individual patients. In particular, women have an elevated risk of experiencing CINV as do younger patients and those who don’t drink much alcohol. A history of morning sickness or previous CINV can also increase a patient’s individual risk of CINV
45
. These risk
factors are well established, and there have been relatively few further studies in recent years. Leading treatment guidelines recommend that the choice of antiemetic prophylaxis is primarily guided by the emetogenicity of the chemotherapy regimen, rather than patient-related risk factors. However, some guidelines recommend that these factors should be taken into account in individual treatment decisions, although more research is necessary to establish the effect of such an approach on overall treatment outcomes 10.
17
Introduction 1.8.Prophylaxis and treatment options 1.8.1 Neurophysiology Evidence accumulating in recent years has shown that the activation of neurotransmitters via peripheral and central pathways highly influences the development of CINV. As a result, treatment of CINV focuses on the modulation of neurotransmitter and receptor systems
49
. While numerous
neurotransmitters may contribute to the vomiting response, two of the most clinically important are 5-HT and substance P. The activation of these influences the development of CINV at different phases (acute and delayed, respectively) and may therefore be used to guide treatment decisions or influence drug selection (Table 2) 36.
1.8.2. Historical Perspectives Antiemetic prophylaxis has been improving continuously over the past decades. In the past, patients receiving cisplatin would frequently be admitted and heavily sedated with lorazepam; in contrast, with modern antiemetics and a shift towards less highly emetogenic chemotherapies (eg, carboplatin rather than cisplatin), many fewer patients require admission and antiemetic outcomes have improved dramatically. Corticosteroids were first found to have antiemetic properties more than 30 years ago 35. As research gradually revealed more about the mechanisms and signaling systems involved in CINV, a 18
Introduction growing number of therapeutic targets were identified. An initial focus on the dopamine system pointed to the use of Phenothiazines and Butyrophenones. Subsequently, studies of the 5-HT3 receptor in particular proved to be a key advance, and the introduction of 5-HT3 antagonists in the 1990s is often heralded as one of the most significant advances in the treatment of CINV
50
.
The emergence of the NK-1 receptor antagonist aprepitant in 2003 followed by development of novel delivery mechanisms and combination regimens for 5HT3 antagonists, represent key recent developments in this field.
1.8.3.Agents and Evidence Given the involvement of several neural systems in the pathophysiology of CINV, it is logical to consider targeting any or all of these systems for prevention of nausea and vomiting. Consequently, a wide array of antiemetic agents from several different classes is in common use (Table 3)35. Beyond specific agents, consideration may be given to alternative delivery formulations. More drugs are becoming available in forms other than IV, including more oral forms and a broadening array of transmucosal and transdermal delivery methods. In the case of antiemetics, the growing choice of delivery options offers improved flexibility to meet the needs of each individual patient. For example, the transdermal formulation of granisetron adds an extra option for sustaining therapeutic drug levels over many days in patients receiving multi-day chemotherapy, and as an alternative to IV therapy for patients unable to swallow 48
19
Introduction
20
Introduction
Management according to classification 1.9. Chemotherapy drug emetogenicity The management of CINV has been greatly facilitated by the development of classification schemes that reflect the likelihood of emesis developing following treatment with particular agents. A 1997 classification scheme gained broad acceptance and was utilized as the basis for treatment recommendations by guideline panels 36. A modification of this schema was proposed at the 2004 Perugia Antiemetic Consensus Guideline meeting
45
. Chemotherapy agents were divided into four
categories: ●Highly emetic – >90 percent risk of emesis ●Moderately emetic – >30 to 90 percent risk of emesis ●Low emetogenicity – 10 to 30 percent risk of emesis ●Minimally emetic – <10 percent risk of emesis This drug classification schema is utilized in both the updated antiemetic guidelines of the Multinational Association of Supportive Care in Cancer and the American Society of Clinical Oncology 52-54. For combination regimens, the emetic level is determined by identifying the most emetic agent in the combination and then assessing the relative contribution of the other agents. As an
example, cyclophosphamide and doxorubicin are
both
moderately
emetogenic agents, but when given together, the regimen is highly emetic
52, 53
.
In updated antiemetic guidelines from ASCO, combined anthracycline and cyclophosphamide regimens have been reclassified as highly emetic 53.
21
Introduction 1.9.1. Acute emesis Extensive clinical trials have evaluated the 5-HT3 receptor antagonists, the NK1 receptor antagonists, and glucocorticoids in patients with acute and delayed CINV. These trials have focused primarily on patients receiving either highly or moderately emetic intravenously administered chemotherapy regimens. Although not all antiemetic regimens have been evaluated with all chemotherapy combinations, it is reasonable to extrapolate data to other chemotherapy regimens of comparable emetogenicity54. 1.9.1. A. 5-HT3 receptor antagonists A key advance in the prevention of CINV was the development of selective type three 5-hydroxytryptamine (5-HT3) receptor antagonists, a drug class that has a high therapeutic index for prevention of CINV 36.Randomized trials have shown that single-agent 5-HT3 receptor antagonists are more effective than less specific agents such as high-dose metoclopramide and as effective as the combination of high-dose metoclopramide and dexamethasone. When 5-HT3 antagonists are used in combination with dexamethasone, they are more effective than high-dose metoclopramide plus dexamethasone 55. In addition to increased efficacy, these agents are easier to administer and are associated with significantly fewer serious side effects than the less specific serotonin inhibitor metoclopramide. Five
first-generation
5-HT3
receptor
antagonists
(dolasetron, granisetron, ondansetron, ramosetron, and tropisetron) and one second-generation agent (palonosetron) are available. An orally disintegrating formulation of ondansetron also is available that disperses rapidly when placed on the tongue and does not need to be swallowed with water
56
. This
formulation may be particularly useful for patients with dysphagia or anorexia. A granisetron transdermal system is also available.
22
Introduction First-generation agents A large number of randomized trials have clarified the properties of the firstgeneration 5-HT3 receptor antagonists. Key findings include the following: ●The first-generation 5-HT3 receptor antagonists all appear equally effective at preventing CINV at the recommended doses. A meta-analysis has shown no clear advantage for either ondansetron or granisetron in the prophylaxis of acute or delayed emesis 57. ●There is a plateau in therapeutic efficacy at a definable dose level for each drug, and further dose escalation does not improve outcome58. ●A single dose of a 5-HT3 receptor antagonist prior to chemotherapy is therapeutically equivalent to a multiple dose schedule 59. ●The efficacy of 5-HT3 receptor antagonists is significantly improved when they are combined with glucocorticoids. ●Oral formulations of these agents are as effective as intravenous formulations 60.
ECG interval changes and cardiac arrhythmias EKG interval changes are a class effect of the first-generation 5-HT3 antagonists, including ondansetron,granisetron and dolasetron, although they have not been reported with transdermal granisetron. EKG interval changes appear to be most prominent one to two hours after a dose of these agents, are mostly small and clinically insignificant, and return to baseline within 24 hours 61
. However, potentially fatal cardiac arrhythmias, including torsade to pointes,
have been reported in association with QTc prolongation. The following sections describe the warnings/precautions regarding cardiotoxicity of these agents from the US Food and Drug Administration (FDA)62.
23
Introduction Dolasetron Due to the risk of QTc prolongation from increased drug exposure, the injection form of dolasetron is contraindicated for prophylaxis of CINV in both children and adults
63
. The risk of developing an abnormal heart rhythm with
oral dolasetron is less than that seen with the injection form. However, there is still a potential risk. The
FDA
recommends
the
following
precautions
in
patients
receiving oral dolasetron 63: ●Potassium and magnesium levels should be assessed, and if abnormal, corrected before initiation of treatment with dolasetron. These electrolytes should be monitored after administration as clinically indicated. ●Use electrocardiographic monitoring in patients with heart failure, a slow heart rate, underlying cardiac disease, the elderly, and in patients with renal impairment. ●Use of dolasetron should be avoided in patients with congenital long-QT syndrome. ●Drugs known to prolong the PR (eg, verapamil) or QRS interval (eg, flecainide, quinidine) should be avoided in patients taking dolasetron. Because of these risks, dolasetron (both oral and IV) has been removed from the market in Canada, but remains available elsewhere. Ondansetron Food and Drug Administration has issued a warning about QTc prolongation and potentially fatal cardiac arrhythmias in patients treated with ondansetron. QT prolongation occurs in a dose-dependent manner and specifically at a single IV dose of 32 mg. QT interval prolongation is expected to be greater with faster rate of infusion and larger doses for IV administration63.
24
Introduction Revised labeling in the US includes a recommendation to limit single IV doses to no more than 16 mg, avoid use of ondansetron in patients with congenital long-QT syndrome, and to use ECG monitoring in certain patients, including those with hypokalemia or hypomagnesemia, heart failure, bradyarrhythmias, and in patients taking other medications that increase the risk of QTc prolongation. Canadian guidelines that took effect in June 2014 place additional dosing restrictions on IV ondansetron to mitigate the risk of QT prolongation in the elderly 63: ●In patients ≥75 years of age, the initial IV dose should not exceed 8 mg. ●For patients
a
single
agent, palonosetron is
more
effective
than ondansetron or dolasetron at preventing emesis due to moderately emetic chemotherapy 67. This was illustrated by a multicenter trial in 592 patients, the majority of whom received doxorubicin and cyclophosphamide for breast cancer. Subjects were randomly assigned to a single IV dose of palonosetron at 25
Introduction one of two dose levels (0.25 or 0.75 mg IV) or dolasetron (100 mg)
65
. More
patients treated with palonosetron (0.25 mg) had complete control of both acute (63 versus 53 percent) and delayed emesis (54 versus 39) compared with dolasetron. A dose of 0.75 mg was not significantly superior compared with 0.25 mg 65. When used in combination with glucocorticoids, palonosetron provides superior control of delayed emesis compared with first-generation 5-HT3 receptor antagonists combined with glucocorticoids. ●In
a
phase
III
double-blind,
double-dummy
trial,
1143
patients
receiving cisplatin or an anthracycline/cyclophosphamide combination
were
randomly assigned todexamethasone plus either palonosetron or granisetron on day 1 prior to chemotherapy; all patients received dexamethasone on days 2 and 3
66
. During the acute phase, the rate of complete control of CINV was
similar (75 versus 73 percent with palonosetron and granisetron, respectively), but during the delayed phase (24 to 120 hours), complete responses occurred in significantly more patients receiving palonosetron (57 versus 45 percent). An unresolved question arising from this study design is whether the efficacy differences noted would have persisted with the addition of aprepitant, which all evidence-based guidelines recommend in this setting66. ●In a second phase III trial, in which 667 patients receiving cisplatin-based chemotherapy were randomly assigned to palonosetron (0.25 mg), palonosetron (0.75 mg), or ondansetron (32 mg), no significant differences in antiemetic control were noted between palonosetron and ondansetron67. Approximately two-thirds of patients received concomitant dexamethasone.In this subset of patients, complete response rates were numerically higher in both palonosetron arms compared to ondansetron during the first 24 hours. During the delayed (24 to 120 hours) phase, complete response was significantly higher on the 0.25 mg
26
Introduction palonosetron arm compared with the ondansetron arm (42 versus 29 percent, p = 0.021) 67. Updated antiemetic guidelines from the American Society of Clinical Oncology (ASCO) recommend palonosetron as the preferred 5-HT3 antagonist for patients who receive moderately emetic chemotherapy53, 54. A non-inferiority trial documented similarity between the oral and IV formulations and validated the correct dose (0.5 mg oral) (table 3). The oral formulation ofpalonosetron, which was approved by the FDA in 2008, is not marketed in the United States but is available in a number of European countries. Adverse effects 5-HT3 receptor antagonists are generally safe, with a favorable side effect profile (predominantly low grade headache, malaise, and constipation). A few reports have appeared suggesting a potential link between 5-HT3 receptor antagonists and the serotonin syndrome, which is caused when serotonin accumulates to high levels in vivo. Symptoms include confusion, agitation, restlessness, muscle twitching or stiffness, fever, sweating, fluctuations in heart rate and blood pressure, as well as nausea and/or vomiting, loss of consciousness, and coma; the syndrome can be fatal if not treated. However, in nearly all cases, the use of concomitant medications with the 5HT3 receptor antagonist has limited the ability to establish a definitive association. Nevertheless, caution is advised when using 5-HT3 receptor antagonists in combination with other drugs that affect serotonin levels68.
2.9.1. B. Neurokinin-1 receptor antagonists
27
Introduction The
introduction
of
the
NK1
receptor
(NK1R)
antagonists aprepitant and fosaprepitant (a parenteral water-soluble prodrug of aprepitant that is effective as a one-day treatment have significantly improved the ability to prevent both acute and delayed CINV in patients receiving highly and moderately emetic chemotherapy. Casopitant is another NK1R antagonist that can be given as a single day 1 oral dose or in a mixed intravenous plus oral three-day schedule in conjunction with dexamethasone and ondansetron; it is not yet commercially available in any country. Aprepitant and fosaprepitant Efficacy The benefit of combining an NK1R antagonist (aprepitant, fosaprepitant, or casopitant) with an 5-HT3 receptor antagonist plus a glucocorticoid for the prevention of acute CINV was addressed in a meta-analysis of 17 trials, totaling 8740 patients who were receiving highly or moderately emetogenic chemotherapy
69
. The addition of a NK1R antagonist to standard antiemetic
therapy significantly improved the rate of complete response (CR, absence of emesis and no need for rescue antiemetics) in both the overall phase (during the first 120 hours of chemotherapy, 72 versus 54 percent, odds ratio [OR] 0.51, 95% CI 0.46-0.57) and in the acute (first 24 hours, OR 0.56, 95% CI 0.48-0.65) as well as delayed phase (OR 0.48, 95% CI 0.42-0.56). For other secondary outcomes (rate of emesis, absence of nausea), the addition of an NK1R antagonist was also superior to the control arm. In subgroup analyses, benefit was seen for both highly emetogenic (CR, 73 versus 54 percent, OR 0.46, 95% CI 0.40-0.53) and moderately emetogenic chemotherapy (CR 71 versus 54 percent, OR 0.59, 95% CI 0.61-0.67). There appeared to be no differences in treatment efficacy for aprepitant/fosaprepitant and casopitant. The use of an NK1R antagonist did not increase the risk of diarrhea, although rates of hiccups and fatigue/asthenia were significantly higher. There was a suggestion that use 28
Introduction of an NK1R antagonist increased the risk of a severe infection (6 versus 2 percent in a pooled analysis of three trials); however, this was not associated with an increased rate of neutropenia or febrile neutropenia69. Need for a 5-HT3 agent Aprepitant and fosaprepitant improve control of CINV when combined with a 5-HT3 receptor antagonist and dexamethasone. Aprepitant plus dexamethasone alone is not as effective as the three-drug combination regimen. A 5-HT3 receptor antagonist remains necessary, at least in patients receiving cisplatinbased chemotherapy. This
was
illustrated
by
a
randomized
trial
in
which
patients
receiving cisplatin chemotherapy were randomly assigned to the combination of aprepitant plus granisetron, granisetron, or aprepitant (on one of two schedules)
70
. All patients also received dexamethasone (20 mg orally) before
cisplatin. While the three-drug combination blocked emesis in 80 percent of patients, dexamethasone plus either granisetron or aprepitant was effective in only 57 percent and 43 to 46 percent of cases, respectively 70. One- versus three-day administration In the United States, both aprepitant and fosaprepitant are approved for use in three-day schedules. However, a single-day dosing schedule for fosaprepitant was approved by the FDA based upon the results of a phase III trial involving 2247 patients receiving single-day cisplatin(>70 mg/m2) based chemotherapy. The control group received aprepitant administered in the standard three-day schedule along with ondansetron plusdexamethasone; this was compared with a single 150 mg dose of fosaprepitant combined with ondansetron on day 1 plus dexamethasone on days 2, 3, and 4. Complete antiemetic response rates were nearly identical between the aprepitant and fosaprepitant arms (72.3 versus 71.9 percent)72. 29
Introduction Issues related to inhibition of CYP3A4 NK1 receptor antagonists such as aprepitant and fosaprepitant are moderate inhibitors of the cytochrome P450 enzyme CYP3A4, which is particularly important in drug metabolism 72. CYP3A4 is responsible for the metabolism of glucocorticoids, and thus the dose of dexamethasone was reduced in clinical trials from 20 mg to 12 mg on day 1 and from 8 mg twice daily to 8 mg daily on days 2 and 3 when given concurrently with aprepitant 73. This dose reduction applies only when glucocorticoids are used as antiemetics in conjunction with NK1 receptor antagonists, not when given as an antitumor component of a chemotherapy regimen. Theoretically, aprepitant could decrease the clearance of drugs metabolized by CYP3A4 (cyclophosphamide, docetaxel, etoposide, irinotecan, vinca alkaloids), resulting in prolonged exposure and increased toxicity. However, there is no clinical evidence that this actually occurs 74.
Netupitant plus palonosetron (NEPA) NEPA is a novel oral fixed dose combination containing 300 mg of netupitant (a highly selective NK1 receptor antagonist) and 0.5 mg of palonosetron, a pharmacologically and clinically distinct 5-HT3 receptor antagonist. At least comparable efficacy and safety of a single dose of NEPA on day 1 in conjunction with dexamethasone has been shown for control of both acute and delayed nausea and emesis after highly or moderately emetogenic chemotherapy compared with aprepitant for three days plus a 5-HT3 receptor antagonist and dexamethasone
75, 76
. These data are described in more detail
below. Based upon these data, NEPA was approved in the United States for prevention of chemotherapy-related nausea and vomiting in October 2014. In 30
Introduction keeping with the updated recommendations from ASCO conjunction
with
a
glucocorticoid,
is
54
an
NEPA, in alternative
to aprepitant and fosaprepitant-containing regimens for patients receiving highly emetogenic chemotherapy such as cisplatin or combined anthracycline plus cyclophosphamide.Like aprepitant and fosaprepitant, netupitant is also an inhibitor of CYP3A4, and a reduced dose of concurrently administered glucocorticoids is needed. Rolapitant Rolapitant is a potent selective NK1 receptor antagonist with a longer plasma half-life (approximately seven days) than either aprepitant orfosaprepitant. Safety and efficacy were established in three randomized, double-blind trials in which rolapitant (180 mg orally one to two hours before chemotherapy administration)
in
combination
with
IV granisetron on
day
1
and dexamethasone (20 mg on day 1 followed by 8 mg twice daily on days 2 to 4 of cycle 1) was compared with a control therapy (placebo with the same dose and schedule of granisetron and dexamethasone) in patients receiving highly emetogenic
(eg, cisplatin,
or
anthracycline
plus cyclophosphamide)
or
moderately emetogenic chemotherapy agents 77. Patients treated with rolapitant had a significantly greater protection from delayed emesis, but there was less consistency in the acute phase of CINV, with the moderately emetogenic trial and one of the highly emetogenic studies failing to show a significant improvement in emesis control within 24 hours of chemotherapy. Rolapitant is approved in adults, in combination with other antiemetic agents, to prevent delayed phase nausea and vomiting associated with initial and repeat courses of emetogenic cancer chemotherapy78.
31
Introduction 1.9.1. C. Glucocorticoids Short courses of glucocorticoids are widely used both as single agents for regimens with low risk of causing CINV and in combination with 5-HT3 receptor
inhibitors and/or NK1
receptor
antagonists
for
more
emetic
chemotherapy regimens. When used in this fashion, glucocorticoids have a high therapeutic index. Although the various glucocorticoids are probably equally effective when used at an appropriate dose, dexamethasone has been the most extensively evaluated and is the most widely used53. Single agent Single agent dexamethasone has been compared with either placebo or no treatment in a number of randomized trials. A meta-analysis of 32 randomized trials evaluated 5613 patients who received moderately or highly emetogenic chemotherapy 79. Dexamethasone was superior to placebo or no treatment for complete protection from both acute emesis (risk ratio [RR] 1.30) and delayed emesis (RR 1.30). However, dexamethasone as a single agent is insufficient to control CINV in most of these patients 53. Combination with a 5-HT3 antagonist Glucocorticoids alone represent insufficient first-line therapy for patients receiving either moderate or highly emetic chemotherapy agents. However, the antiemetic efficacy of the 5-HT3 receptor antagonists is significantly enhanced by the addition of a glucocorticoid 80. Benefit for combined therapy was shown in a meta-analysis of 3791 patients enrolled in 22 randomized trials in which a 5-HT3 receptor antagonist plusdexamethasone was compared with a 5-HT3 antagonist plus placebo or no treatment in patients receiving moderate or highly emetic chemotherapy 79. The pooled risk ratio for emesis protection was 1.25, indicating that the addition of dexamethasone increased the chance of no acute vomiting by 25 percent. 32
Introduction Dose The impact of glucocorticoid dose was explored in a double-blind trial that randomly assigned 531 patients receiving cisplatin ≥50 mg/m2 to one of four intravenous doses of dexamethasone administered by a 15-minute infusion prior to cisplatin administration. All patients received 8 mg of ondansetron as well. At doses of 20, 12, 8, and 4 mg, complete protection from vomiting was achieved in 83, 79, 69, and 69 percent of patients, respectively, and nausea was prevented in 71, 67, 61, and 61 percent81. The optimal dose of dexamethasone for highly to moderately emetic chemotherapy not containing cisplatin was evaluated by the Italian Group for Antiemetic Research
82
. In this trial, all patients received IV ondansetron and
were randomized to one of three schedules of dexamethasone (either 8 or 24 mg IV prior to chemotherapy, or 8 mg IV before treatment followed by 4 mg every six hours). Rates of complete protection from acute or delayed emesis were similar among the groups, and the authors concluded that a single 8 mg IV dose prior to chemotherapy represented the appropriate dexamethasone regimen.As noted above, the dose of dexamethasone is reduced when it is in combination with an NK1 receptor antagonist82.
1.9.1. D. Other agents Other agents that have been used in the treatment or prevention of CINV include
phenothiazines
(eg, prochlorperazine), metoclopramide,
butyrophenones, and cannabinoids. These agents have a lower therapeutic index than the 5-HT3 receptor antagonists, NK1R antagonists, and glucocorticoids for highly or moderately emetogenic chemotherapy regimens. Their use should be restricted to patients who are intolerant of or refractory to these first line agents. The benefits of synthetic oral cannabinoids in this setting 33
Introduction remain controversial given the lack of evidence on their safety and efficacy 83. Phenothiazines
could
be
used
as
an
alternative
to
single
agent dexamethasone for those receiving chemotherapy with a low risk of emesis, if a glucocorticoid is contraindicated 53. Other drugs that may be useful as adjuncts to conventional antiemetic agents include lorazepam and diphenhydramine. These are not recommended as single agent antiemetics53. 1.9.2. Delayed emesis Delayed emesis is defined by its occurrence more than 24 hours after chemotherapy. Although it is most common following high-dose cisplatin86, delayed emesis may occur with other agents as well 59. Regimens with a high risk of delayed emesis The risk of delayed emesis after cisplatin (doses >70 mg/m2) ranges between 60 and 90 percent in the absence of effective prophylaxis. The risk of delayed emesis without any prophylaxis is estimated to be between 20 and 30 percent in patients
receiving
chemotherapy
with
an
anthracycline
plus cyclophosphamide 85.Although the risk of delayed emesis has been best studied
with
high-dose cisplatin and
the
combination
of doxorubicin plus cyclophosphamide, other moderately emetogenic agents are also associated with delayed emesis. These include doxorubicin ≥40 mg/m2 as a single agent or ≥25 mg/m2 in combination with other chemotherapeutic
agents
cyclophosphamide), epirubicin ≥75 mg/m2 as
(especially a
single
agent
or
≥50 mg/m2 when given in combination with other agents, combinations of cyclophosphamide
≥600 mg/m2 in
combination
drugs, carboplatin ≥300 mg/m2, oxaliplatin (as
used
in
with the
other FOLFOX
[oxaliplatin plus short-term infusional fluorouracil and leucovorin] regimen for 34
Introduction advanced colorectal cancer), and cisplatin at doses between 20 and 50 mg/m2 59. One study found that among 68 patients treated with one of these regimens who had no post-chemotherapy vomiting in the 24 hours after administration of prechemotherapy ondansetronand dexamethasone, 28 (41 percent) vomited in the next four days when no further antiemetics were given 61
. This frequency was reduced to 15 of 75 (20 percent) when ondansetron was
continued. Management Many of the regimens associated with delayed emesis are classified as highemetic risk, and guidelines from the American Society of Clinical Oncology (ASCO)
recommend
the
use
of
an
NK1
receptor
antagonist
(either aprepitant on days 1 to 3, fosaprepitant on day 1 only, or rolapitant on day 1 only), plus a glucocorticoid on days 1 to 4, and a 5-HT3 receptor antagonist on day 1
53
. NEPA (a fixed combination of the NK1 receptor
antagonist netupitant pluspalonosetron) in conjunction with a glucocorticoid, is an additional option in this setting
54
. This regimen is effective against both
acute and delayed emesis. 1.9.2. A. Glucocorticoids The value of maintenance therapy with oral glucocorticoids following treatment of acute CINV was shown in patients treated with cisplatin-based chemotherapy regimens in at least two randomized trials
86
. However,
glucocorticoids alone are often not sufficient to prevent delayed emesis in patients receiving cisplatin. 1.9.2. B. NK1 receptor antagonists The benefit of adding an NK1R antagonist (aprepitant, fosaprepitant, or casopitant) to dexamethasone and a 5-HT3 antagonist for prevention of delayed emesis in patients receiving highly or moderately emetogenic chemotherapy 35
Introduction was shown in a meta-analysis of 17 trials and described above. Importantly, the addition of NK1R antagonists increased control rates in the overall phase (ie, 120 hours after chemotherapy) independently of whether ondansetronwas used in the control arm beyond day 1 or not. However, patients who did not use ondansetron after day 1 seemed to have a greater benefit from the addition of the NK1R antagonist69.
Aprepitant versus glucocorticoids in patients receiving Doxorubicin plus Cyclophosphamide The doxorubicin plus cyclophosphamide (AC) regimen used in patients with breast cancer is considered to have a high risk of both acute and delayed emesis.
As
such,
ASCO
recommend aprepitant plusdexamethasone for (dexamethasone
alone
if fosaprepitant is
53
and NCCN guidelines the
used
delayed on
day
period 1).
These
recommendations represent an extrapolation from data fromcisplatin trials, in which aprepitant plus dexamethasone in the delayed phase was better than dexamethasone alone 69. The role of dexamethasone only in the delayed phase was directly addressed in a trial in which patients receiving AC for breast cancer were randomly assigned to oral dexamethasone (4 mg twice daily) or aprepitant (80 mg once daily) on days 2 and 3; all patients received IV palonosetron 0.25 mg, dexamethasone 8 mg, and aprepitant 125 mg on day 1 87. From days 2 to 5, the primary end points, complete response rates (defined as no vomiting and no rescue treatment) were the same with both antiemetic regimens (79.5 percent), as were secondary endpoints (which included no nausea). The incidence rates of insomnia (2.9 versus 0.4 percent) and heartburn (8.1 versus 3.6 percent) were significantly greater with dexamethasone on days 2 to 587.
36
Introduction These data suggest that for patients receiving aprepitant, a 5-HT3 antagonist, and dexamethasone therapy on day 1, dexamethasone is as effective in the delayed period as is aprepitant, and it could be considered in such patients, particularly in resource-limited settings. What is not clear is whether the combination
of
delayed
phase
aprepitant
plus
dexamethasone,
or fosaprepitant on day 1 followed by delayed phase dexamethasone is even better than aprepitant on day 1 followed by dexamethasone alone for the delayed period69. Aprepitant versus metoclopramide plus dexamethasone in patients receiving cisplatin All of the trials examining the benefit of aprepitant to prevent delayed CINV used a three-day schedule of administration, in conjunction with oral glucocorticoids. Single day administration is approved for fosaprepitant but not aprepitant. The use of metoclopramide as a substitute for aprepitant on days 2 and 3 was addressed in a randomized trial in which 303 previously untreated patients received acisplatin-based chemotherapy regimen
90
. All patients
received the same regimen to prevent acute emesis on day 1 (aprepitant 125 mg, dexamethasone 8 mg, andpalonosetron 0.25 mg) and were randomly assigned to dexamethasone 8 mg daily plus either metoclopramide 20 mg four times a day or aprepitant 80 mg daily, on days 2 and 3. The primary endpoint was complete response (no vomiting or rescue medication on days 2 through 5 after chemotherapy). The complete response rate was not significantly different (80.3 versus 82.5 for aprepitant and metoclopramide, respectively) as were all secondary endpoints, including no nausea, and adverse events were not significantly different. The authors concluded that aprepitant was not superior to metoclopramide for control of delayed emesis after cisplatin when used in conjunction with dexamethasone after day 1 of chemotherapy88.
37
Introduction Given that many institutions have switched over to day 1 single dose fosaprepitant followed by dexamethasone alone on days 2 to 3 rather than three-day aprepitantplus dexamethasone to prevent delayed emesis, the relevance of these results to current clinical practice is unclear. Rolapitant Rolapitant is a potent selective NK1 receptor antagonist with a longer plasma half-life (approximately seven days) than either aprepitant orfosaprepitant. Safety and efficacy were established in three randomized double-blind trials in which rolapitant (180 mg orally one to two hours before chemotherapy administration) in combination with granisetron (10 mcg/kg IV on day 1) and dexamethasone (20 mg on day 1 followed by 8 mg twice daily on days 2 to 4 of cycle 1) was compared with a control therapy (placebo with the same dose and schedule of granisetron and dexamethasone) in a total of 2800 patients receiving
highly
emetogenic
(eg, cisplatin or
combined
anthracycline
plus cyclophosphamide) or moderately emetogenic chemotherapy 77, 78. Patients treated with rolapitant had a significantly greater reduction in delayed vomiting and use of rescue medication for nausea and vomiting in patients receiving both highly emetogenic and moderately emetogenic chemotherapy. There was less consistency in the acute phase of CINV (up to 24 hours after chemotherapy), and as has been seen with other NK1 receptor antagonists, nausea was not as well
controlled
as
emesis
Unlike aprepitant and fosaprepitant,
in
the which
groups are
receiving
moderate
rolapitant.
inhibitors
of
CYP3A4, rolapitant does not inhibit this metabolic pathway, and therefore no adjustment ofdexamethasone dose is required. Rolapitant does inhibit the CYP2D6 enzyme, which is responsible for metabolizing certain drugs such as thioridazine; the use of both drugs together is not recommended 54. Rolapitant is approved in adults, in combination with other antiemetic agents, to prevent delayed nausea and vomiting associated with the initial and repeat 38
Introduction courses of emetogenic cancer chemotherapy. No clinical trials have yet reported a definitive direct comparison of any of the available NK1 receptor antagonists78. NEPA NEPA is a novel oral fixed dose antiemetic combination containing 300 mg of netupitant (a highly selective NK1 receptor antagonist) and 0.5 mg of palonosetron, a pharmacologically and clinically distinct 5-HT3 receptor antagonist. In conjunction with a glucocorticoid, NEPA is an alternative to aprepitant and fosaprepitant-containing regimens for patients receiving highly
emetogenic
chemotherapy
anthracyclinepluscyclophosphamide.Single
such dose
as cisplatin or NEPA
in
combined conjunction
with dexamethasone for control of both acute and delayed nausea and emesis has
been
compared
with palonosetron plus
dexamethasone
and aprepitant plus a 5-HT3 receptor antagonist and dexamethasone
75
89
in three
trials conducted in populations receiving either moderately or highly emetogenic chemotherapy: ●In a phase II dose finding study, 694 patients receiving cisplatin-containing chemotherapy were randomly assigned to NEPA at one of three different oral doses (100, 200, or 300 mg) plus palonosetron 0.5 mg on day one, palonosetron only (0.5 mg), or standard three-day aprepitant plus IV ondansetron; all patients received dexamethasone on days 1 through 4 [47]. Each dose of NEPA provided superior prevention of CINV, with the highest NEPA dose showing the greatest incremental benefit (complete protection from emesis and no rescue medication needed through hour 120 in 87, 88, and 90 percent of patients treated with 100, 200, and 300 mg of netupitant, respectively, compared with 77 percent for palonosetron alone, and 87 percent for aprepitant plus 5-HT3 antagonist). Adverse events were comparable across groups75.
39
Introduction ●Efficacy of NEPA over multiple cycles of chemotherapy was evaluated in a phase III randomized trial in which 413 patients receiving a variety of moderately (carboplatin, oxaliplatin, doxorubicin, cyclophosphamide, irinotecan, epirubicin , daunorubicin) or highly emetogenic (cisplatin, dacarbazine carmustine) chemotherapy were randomly assigned to NEPA given on day 1 with oral dexamethasone versus
a
three-day
of aprepitant plus palonosetron and
dexamethasone
76
.
regimen In
both
groups,
dexamethasone was administered on days 1 through 4 for highly emetogenic chemotherapy and on day 1 only for moderately emetogenic chemotherapy. During cycle 1, complete response rates (no emesis and no need for rescue medication through hour 120) were 81 versus 76 percent for NEPA and aprepitant/palonosetron, respectively,
and
antiemetic
efficacy
was
maintained over multiple cycles. The NEPA group showed a small but consistent numerical advantage (2 to 7 percent) over aprepitant and palonosetron during all cycles. The incidence and type of adverse events was similar in both group. Although these two trials included arms comparing NEPA versus a threeday aprepitant-containing regimen, neither trial was designed to provide a definitive comparison of the relative efficacy of NEPA and the aprepitantcontaining regimen89. ●The third trial compared NEPA versus palonosetron alone in 1455 patients receiving cyclophosphamide plus
an
anthracycline
(either doxorubicin or epirubicin); all patients also received dexamethasone on day 1 only
89
. The percentage of patients with a complete response (through
hour 120) was significantly higher with NEPA (74 versus 67 percent, p = 0.001). NEPA was well tolerated and had a similar safety profile to
40
Introduction palonosetron. Based upon these data, NEPA was approved in the United States for prevention of chemotherapy-related nausea and vomiting in October 2014 77. An important point
is
that
if
NEPA
is
used
in
the
setting
of
anthracycline
plus cyclophosphamide chemotherapy routine maintenance antiemetic therapy is not recommended after day 1. If used with a cisplatin-containing regimen, dexamethasone is recommended on days 1 through 4. 1.9.2. C. 5-HT3 antagonists alone Conflicting results have been described with the use of first generation 5-HT3 receptor antagonists as single agents for protection against delayed emesis
90
.
Although some benefit has been seen when these agents are used as monotherapy, the benefit has not been as great as that seen with glucocorticoids. Furthermore, continuing a 5-HT3 receptor antagonist beyond 24 hours along with glucocorticoids did not confer additional benefit compared to corticosteroids alone. Thus, the use of the 5-HT3 receptor antagonists as a sole
maneuver
to
prevent
delayed
emesis
in
patients
receiving cisplatin is notrecommended. The second generation 5-HT3 receptor antagonist palonosetron seem to be superior to other 5-HT3 receptor antagonists for the treatment of delayed emesis due tocisplatin-based chemotherapy: ●In
a
phase
III
trial
of
patients
receiving cisplatin-based
chemotherapy, palonosetron (at one of two doses, either 0.25 mg or 0.75 mg) yielded higher rates of emetic control compared with ondansetron in preventing delayed emesis (complete response rates of 45 and 48 versus 39 percent, respectively), although the results were not statistically significant 67. However, in a subset analysis, palonosetron 0.25 mg was superior to ondansetron for
41
Introduction control
of
delayed
and
overall
emesis
in
patients
receiving
concomitant dexamethasone 67. ●The superiority of palonosetron for prevention of delayed emesis was also shown
in
another
phase
III
trial
in
which
1114
receiving cisplatin orananthracycline/cyclophosphamide combination
patients were
randomly assigned to a single dose of palonosetron or granisetron 30 minutes prior to chemotherapy with all patients receiving dexamethasone for three days 66
. Significantly better control of delayed emesis was achieved in both the
cisplatin and AC subgroups on the palonosetron arm (complete response 57 versus 45 percent with granisetron).Although these results suggest the superiority of palonosetron over other 5-HT3 antagonists for the prevention of delayed emesis, it is unclear whether this difference would persist with the addition of an NK1 receptor antagonist. To date, there are no randomized trials in which the combination of palonosetron and an NK1 receptor antagonist has been compared with a first generation 5-HT3 receptor antagonist plus an NK1 receptor antagonist89. Olanzapine Conventional antiemetics are more successful at preventing emesis than in preventing nausea, particularly delayed nausea. The superiority of the antipsychotic olanzapine over aprepitant for the prevention of delayed nausea was
suggested
in
a
phase
III
trial
conducted
receiving cisplatin ordoxorubicin plus cyclophosphamide 91.
in
247 Patients
patients were
randomly assigned to olanzapine (10 mg orally on the day of chemotherapy, and then 10 mg once daily on days 2 through 4), or aprepitant (125 mg orally prior to chemotherapy, followed by 80 mg orally on days 2 and 3), both in combination with palonosetron (0.25 IV on the day of chemotherapy) plus dexamethasone. Dexamethasone (20 mg) was only given on the day of chemotherapy, while the aprepitant group received dexamethasone 12 mg on 42
Introduction the day of chemotherapy followed by dexamethasone 4 mg twice daily on days 2 and 3. Following cycle 1, rates of prevention of acute nausea (87 percent in both the olanzapine and aprepitant groups), and of complete control of acute (97 versus 87 percent) and delayed vomiting (77 versus 73 percent) were similar. However, patients treated with olanzapine had a significantly higher rate of nausea control in the delayed period (69 versus 38 percent). The results were maintained
during
cycles
2
to
4.Superiority
over
extended
duration dexamethasone was also suggested in a second trial involving 229 patients receiving moderately or highly emetogenic chemotherapy
92
. All
patients received a 5-HT3 antagonist plus decadron on day 1, and they were randomly assigned to olanzapine 10 mg orally daily on days 1 to 5, or dexamethasone 10 mg IV once daily on days 2 to 5. Complete response rates for acute emesis were similar (91 versus 89 percent); the likelihood of a complete delayed response was higher with olanzapine (79 versus 57 percent), but this difference did not reach the level of statistical significance. Delayed nausea control was also significantly greater with olanzapine (70 versus 30 percent).While these data are intriguing, these findings need to be replicated in a larger study. Olanzapine may also be useful for management of breakthrough emesis 91. 1.9.3. Moderate risk agents The incidence of delayed emesis following treatment with moderate risk agents other than the combination of cyclophosphamide plus an anthracycline is not well characterized. Other cyclophosphamide or doxorubicin-based regimens, as well as carboplatin and oxaliplatin, can cause delayed emesis. The contribution of NK1 receptor antagonists such as aprepitant or fosaprepitant to the control of delayed emesis with moderate risk agents was shown in a meta-analysis and is described above
69
. Furthermore, benefit from the novel oral fixed dose 43
Introduction combination NEPA (netupitant plus palonosetron) in patients treated with a carboplatin-containing regimen was shown in one of the phase III registration trials 89. Glucocorticoids
are
also
consistently
useful
agents.
The
value
of
maintenance dexamethasone was demonstrated in a randomized placebo controlled trial of patients undergoing cyclophosphamide-based chemotherapy 84
. In this trial, 98 patients were given granisetron and dexamethasone before
chemotherapy and randomized to receive either oral dexamethasone 4 mg twice daily as maintenance or no maintenance. Maintenance dexamethasone was associated with a higher rate of complete (57 versus 33 percent) and major control (33 versus 15 percent) of delayed emesis. The 5-HT3 receptor antagonists also have activity as single agents for delayed emesis with cyclophosphamide-based chemotherapy
59
. However, there is no
evidence that they are superior to dexamethasone alone or that combination therapy with dexamethasone is superior to dexamethasone alone 85. A randomized trial of 708 patients receiving moderately emetogenic chemotherapy and concurrent antiemetics illustrates the relative roles of dexamethasone and 5-HT3 receptor antagonists in the management of delayed emesis 85: ●Patients without acute nausea or vomiting (the low-risk group) were randomized to receive dexamethasone (4 mg orally twice daily on days 2 through 5) plusondansetron (8 mg orally twice daily on days 2 through 5), dexamethasone alone on the same schedule, or a placebo. Among these 618 patients, there was a complete absence of delayed nausea and vomiting in 92, 87, and 77 percent of patients in the combined therapy, dexamethasone, and placebo groups, respectively. Protection with dexamethasone alone or with dexamethasone plus ondansetron was better than that with placebo; however, the combination was not statistically superior to dexamethasone alone. 44
Introduction ●The key factor in preventing delayed emesis was the control of acute symptoms following chemotherapy. Patients who had either vomiting or moderate to severe nausea in the 24 hours following chemotherapy constituted a high-risk group. These 87 patients were randomly assigned to oral dexamethasone alone or in combination with ondansetron, at the same doses and schedules as in the low-risk group. Despite treatment, complete protection from delayed emesis or moderate to severe was achieved in only 41 and 23 percent of patients treated with the combination and dexamethasone, respectively 85. The relative roles of palonosetron and aprepitant in controlling delayed nausea was studied in a randomized trial of 944 evaluable patients receiving primarily (95 percent) moderately emetogenic chemotherapy
93
. Palonosetron did not
provide superior control of delayed nausea compared with granisetron, when both were provided on day 1 with dexamethasone, and prochlorperazine was administered on days 2 and 3. In addition, aprepitant was not more effective than prochlorperazine when both were combined with dexamethasone on days 2 and 3. 1.9.4. Anticipatory emesis Anticipatory emesis is a conditioned response that occurs in patients who experienced severe nausea and vomiting during prior cycles of chemotherapy 94
. It appears to be induced by sensory cues and cognitive anticipation of
subsequent chemotherapy. Anticipatory nausea has also been described among patients who have a high expectation of developing nausea despite never having received chemotherapy 95. The most effective means to prevent anticipatory nausea or emesis is to ensure good control of acute and delayed emesis, starting from the initial chemotherapy cycle. Once anticipatory emesis has been established,
45
Introduction nonpharmacologic methods (e.g., hypnosis, behavioral therapy with systemic desensitization) may be effective 96. Although few formal trials have been carried out, benzodiazepines before and during chemotherapy may be useful. In one double-blind trial of 57 women undergoing adjuvant chemotherapy for primary breast cancer for example, the addition of low-dose alprazolam (0.5 mg to 2 mg/day) to a psychologic support program including progressive relaxation training was associated with a significantly reduced rate of anticipatory nausea compared with placebo (0 versus 18 percent) 97. 1.9.5 Special situations Consecutive day therapy with highly emetogenic agents When
moderately
or
highly
emetogenic
chemotherapy
agents
(eg, cisplatin, dacarbazine) are administered on several consecutive days, prophylaxis is more difficult. This may be due to anticipatory emesis on the subsequent days of therapy or to the compounding of acute and delayed effects of treatment. Updated American Society of Clinical Oncology (ASCO) antiemetic guidelines suggest that antiemetics appropriate for the emetogenic risk class of the chemotherapy be administered for each day of the chemotherapy and for two days after, if appropriate 53. Trials conducted before the availability of NK1R antagonists suggested that repetitive daily dosing with a 5-HT3 receptor antagonist combined with dexamethasonewas the best approach
98
. However, more recently, the
benefit of adding aprepitant to a 5-HT3 antagonist and dexamethasone was shown in a small trial of 69 patients receiving a five-day cisplatin-containing chemotherapy regimen for germ cell cancer
99
. All patients received a 5-HT3
antagonist (other than palonosetron) once daily on days 1 through 5, plus dexamethasone 20 mg once daily on days 1 and 2, and were randomly assigned 46
Introduction to aprepitant (125 mg on day 3, 80 mg on days 4 and 5) or no aprepitant. The group receiving aprepitant also received dexamethasone 4 mg twice daily on days 6, 7, and 8, while the placebo group received dexamethasone 8 mg twice daily on days 6 and 7, and 4 mg twice daily on day 8. A complete response (no emetic episodes and no use of rescue medication) was noted in significantly more patients receiving aprepitant (42 versus 13 percent), and the visual analog scale score for nausea was numerically lower for aprepitant, although the difference compared with placebo was not statistically significant.Although the authors provided a rationale for starting the NK1R on day 3 rather than on day 1, the optimal schedule for NK1R antagonists for patients receiving consecutive day therapy with highly emetogenic chemotherapy is unknown given the lack of comparative trials addressing this question. For regimens containing five days of cisplatin (eg, for testicular germ cell cancer), we suggest a daily dose of an oral 5-HT3 receptor antagonist plus dexamethasone, with the addition of aprepitant or fosaprepitant starting on day 199. Granisetron transdermal patch A transdermal preparation of granisetron is available (Sancuso) that contains 34.3 mg of granisetron and is designed to deliver 3.1 mg of the drug every 24 hours for up to seven days. The efficacy of the granisetron patch relative to daily oral administration of granisetron was shown in a multinational randomized, double-blind, double-dummy controlled trial in which 641 patients receiving the first cycle of a multiday regimen of either moderately or highly emetogenic chemotherapy were randomly assigned to the patch (applied 24 to 48 hours before the first day of chemotherapy) plus a placebo capsule or to oral granisetron (2 mg daily, one hour prior to chemotherapy on each day of chemotherapy
administration)
plus
a
placebo
patch
100
.
Concurrent
glucocorticoids, which were administered at the investigator's discretion, were given to about 70 percent of the patients in each arm. 47
Introduction The percentage of patients who had complete control of nausea and vomiting until 24 hours after the last chemotherapy dose was not worse with the transdermal patch (60 versus 65 percent with oral granisetron). Fewer than 1 percent of the patches became detached during treatment. In both groups, the most commonly reported toxicities were constipation and headache100. Based upon this trial, the granisetron transdermal system was approved in the United States for the prevention of CINV in patients receiving moderately or highly emetogenic chemotherapy for up to five days. It is recommended that the patch be applied to the upper outer arm a minimum of 24 hours before chemotherapy and removed 24 hours or more after the last chemotherapy dose is administered. It can be worn for up to seven days, depending on the duration of the chemotherapy regimen100.
Induction therapy for acute leukemia High-dose cytarabine regimens (in which cytarabine is administered daily for five or seven days, often with an anthracycline) are the cornerstone of treatment for acute myeloid leukemia. Few studies have addressed the issue of CINV and optimal prophylaxis in this setting of
a
5-HT3
receptor
101
. Although data are lacking, a daily dose
antagonist
(eg, ondansetron 16
mg)
with
or
without dexamethasone appears to be a reasonable option in this setting 101. High-dose chemotherapy regimens The use of high dose chemotherapy in association with a bone marrow or peripheral blood stem cell transplant presents a special challenge to achieving good antiemetic control. The chemotherapy agents employed are often of moderate to high emetogenic risk.
48
Introduction In addition, there are a number of potential factors that can contribute to an increased incidence and severity of CINV in this setting: ●Higher doses of chemotherapy ●Consecutive day administration ●Prior treatment with chemotherapy ●Inclusion of radiation therapy (especially total body irradiation), which has high emetogenic risk ●Associated other medical conditions or medications that may cause emesis There are a limited number of randomized trials specifically studying the issue of emesis in the high dose chemotherapy setting
102
. Most studies have focused
on the combination of a 5-HT3 receptor antagonist and dexamethasone 105. However, a role for aprepitant in this setting is supported by two phase III trials: ●In one trial, 181 patients undergoing a preparative regimen for hematopoietic stem
cell
transplantation
were
to ondansetron plusdexamethasone and
randomly
either aprepitant or
assigned placebo104.
Significantly better emetic control was noted in patients who received aprepitant (no emesis for the entire study period in 73 versus 23 percent of the placebo group), although there were no differences between the groups in use of rescue antiemetics. ●Benefit for aprepitant was also noted in a second phase III trial in which 362 patients with multiple myeloma undergoing autologous HCT after highdosemelphalan were randomly assigned to granisetron plus dexamethasone and either aprepitant or placebo105. Significantly more patients receiving aprepitant achieved the primary end point (no emesis and no need for rescue therapy within 120 hours of administration of high-dose melphalan, 58 versus 41 percent, p = 0.00042). Absence of major nausea (94 versus 88 percent) and 49
Introduction emesis (78 versus 65 percent) within 120 hours also favored the aprepitant group. The 2011 updated antiemetic guidelines from ASCO suggested a 5-HT3 receptor antagonist plus dexamethasone with consideration of aprepitant in this setting 53,54. 1.10. Poor control of emesis Despite the use of appropriate antiemetic prophylaxis, many patients experience clinically significant CINV. Before considering any change in the antiemetic regimen, it is important to exclude other disease- and medicationrelated causes for emesis. Examples include the following: ●The use of opiate analgesics ●Certain antibiotics (eg, erythromycin) ●Central nervous system metastases ●Gastrointestinal obstruction ●Hypercalcemia ●Abdominopelvic radiotherapy Assuming these factors are excluded, it is important to ensure that the patient is receiving the antiemetic appropriate for the drug(s) being given and the correct dose. If the patient was receiving chemotherapy with low emetic risk and is experiencing poor emesis control, it is possible to adjust the regimen to that typically used for a higher risk group. The addition of a benzodiazepine may help to counter increased patient anxiety and possible anticipatory emesis 52. The majority of patients who have breakthrough emesis have derived some benefit from the original antiemetic regimen employed. One or two episodes of emesis withcisplatin is less than ideal but still reflects substantial antiemetic efficacy. Thus, the original antiemetic regimens should usually be retained.Additional
agents
can 50
be
added,
Introduction including lorazepam or alprazolam, olanzapine, a dopaminergic antagonist (eg, prochlorperazine, thiethylperazine, haloperidol), or substituting high-dose 53
intravenous metoclopramide for the 5-HT3 antagonist
. Superiority for
olanzapine (10 mg orally daily for three days) over metoclopramide (10 mg orally three times daily for three days) for treatment of breakthrough nausea and vomiting was shown in a double-blind randomized trial involving 80 patients receiving highly emetogenic chemotherapy
106
. During the 72-hour
observation period, significantly more patients receiving olanzapine had no recurrent emesis (70 versus 31 percent) and no nausea (68 versus 23 percent). Another alternative is to switch to a different serotonin antagonist, since there may be incomplete cross-resistance between agents tested
in
a
double-blind
trial,
in
107
. This approach was
which
patients
who
failed ondansetron plus dexamethasone in the first 24 hours following highly emetogenic chemotherapy were randomly assigned to continue the same treatment or switch to granisetron plus dexamethasone. There was a significantly higher rate of complete protection from emesis in the patients who switched to granisetron (47 versus 5 percent) 107. In other cases, chemotherapy can be altered. Alterations could include single day instead of multiple day therapy, lengthening infusion time, or substituting a less emetogenic agent if such maneuvers do not compromise antitumor activity.
1.11. Cannabinoids and medical marijuana The modest antiemetic activity of cannabinoids and cannabis combined with the relatively unfavorable side effect profile of this class of agents, especially in older patients, has limited their clinical utility. Nevertheless, guidelines from the National Comprehensive Cancer Network (NCCN), ASCO
53
Multinational Association of Supportive Care in Cancer (MASCC)
52
51
, and the state that
Introduction cannabinoids such as dronabinol can be considered for refractory nausea and vomiting and as a rescue antiemetic. Because of medical and legal concerns, the use of medical marijuana is not recommended for management of CINV, and is not included in the most recent guidelines for CINV from the NCCN, ASCO, or MASCC 83. The potential antiemetic utility of cannabinoids was first observed in scattered reports of improved emetic control in patients using marijuana during chemotherapy
108
. While an early prospective uncontrolled pilot study from
1988 found that inhaled cannabis was effective in 78 percent of 56 patients who had inadequate control of nausea and vomiting with the conventional antiemetics that were available at that time 109, there have been no other clinical reports of efficacy of inhaled marijuana and there are no controlled clinical trials comparing marijuana versus other rescue strategies in patients who are refractory to modern antiemetics110. Although concern about the abuse potential of cannabinoid drugs has slowed their development, several cannabinoid-type drugs are commercially available, and others are under study. The two US-approved oral cannabinoids (dronabinol and nabilone) are approved only for chemotherapy-induced nausea and vomiting, and appetite stimulation in wasting illnesses, respectively. An oromucosal spray containing THC plus cannabidiol (and smaller concentrations of other compounds), callednabiximols (Sativex), is approved in Canada and elsewhere (but not yet in the United States) for treatment of neuropathic pain due to multiple sclerosis and as an adjunctive treatment for pain in patients with advanced cancer
111
. It is rapidly absorbed from the buccal mucosa, and the
dose can be self-titrated by the patient. The efficacy of cannabinoids for CINV was addressed in a systematic review of 28 studies (totaling 1772 participants; 9 with dronabinol, 14 with nabilone, 1 fornabiximols, 4 for levonantradol; 2 studies evaluated a combination of 52
Introduction dronabinol plus ondansetron or prochlorperazine)
112
. Eight studies were
placebo-controlled, and three of these also included an active comparator; 20 additional studies included only an active comparator. The most common active comparators were prochlorperazine, chlorpromazine, and domperidone. Risk of bias was high in 23 and unclear for the rest. When taken together, all studies suggested a greater benefit for cannabinoids compared with both the active comparator and placebo, but the benefit was not statistically significant in all studies. Notably, there was a significantly increased risk of short-term adverse effects with cannabinoids, including serious adverse events (OR 1.41, 95% CI 1.04-1.92). Short-term adverse effects included dizziness, dry mouth, nausea, fatigue, somnolence, euphoria, vomiting, disorientation, drowsiness, confusion, loss of balance, and hallucination112.
1.12. Complementary therapies 1.12.1. Ginger Conventional antiemetics are more successful at preventing emesis than in preventing nausea. A total of five randomized placebo-controlled trials have studied the benefit of ginger (Zingiberofficinale) as an aid to reduce nausea during chemotherapy, with mixed results. Three demonstrate benefit while two were completely negative: ●The largest trial randomly assigned 744 patients who experienced nausea following any chemotherapy cycle to placebo, or supplemental ginger (at doses of 0.5, 1, or 1.5 g twice daily) for six days, starting three days prior to the first day of the next two chemotherapy cycles
113
. All patients received a 5-HT3
receptor antagonist on day 1 of all cycles. Two-thirds of the enrolled patients were receiving chemotherapy for breast cancer. All doses of ginger were 53
Introduction associated with a significant reduction in acute nausea throughout day 1 of the chemotherapy cycles, although the largest reduction was seen with the 0.5 and 1 g doses. The authors concluded that ginger supplementation significantly aids in reduction of day 1 nausea during chemotherapy 113. ●A
benefit
for
ginger
root
in
conjunction
with ondansetron and dexamethasone was also shown in a placebo-controlled randomized
trial
of
57
children
and
young
receiving cisplatin/doxorubicin chemotherapy for bone sarcoma
114
adults
. Compared
with conventional antiemetics, the addition of ginger (334 or 800 mg depending on the size of the patient) one hour before, and three and eight hours after the start of chemotherapy significantly reduced the incidence of both acute and delayed emesis. ●A third trial, conducted in 78 women with advanced breast cancer, also demonstrated a reduction in nausea up to 24 hours after chemotherapy from the addition of ginger (1.5 G daily for four days after chemotherapy) to standard antiemetics115. ●However, in contrast to these results, a benefit for ginger in addition to conventional antiemetics (5-HT3 antagonists and/or aprepitant) could not be shown in a randomized, placebo-controlled phase II trial of 162 cancer patients who had suffered CINV during at least one prior cycle of chemotherapy 116. In fact, patients who took ginger plus aprepitant had more severe acute nausea than did those who took only aprepitant. Benefit for ginger was also not confirmed in another trial in which 36 adult cancer patients receiving a cisplatin-based chemotherapy regimen were randomly assigned to standard antiemetics plus ginger capsules (1 G daily) or placebo for three days, and crossed over to the alternative arm for the next cycle of treatment three weeks later
117
. The use of ginger did not improve
either acute or delayed nausea or emesis 117.
54
Introduction
1.12.2. Acupuncture and related therapies Several techniques have been used to stimulate the pericardium 6 (P6 or neiguan) site, which is commonly thought to be useful in the management of chemotherapy-induced nausea and vomiting. These include manual stimulation with the insertion of fine needles (acupuncture), electrostimulation, and noninvasive pressure on the skin over the P6 pressure point (ie, acupressure). Unfortunately, interpretation of the results of randomized trials is hampered by a high risk of bias in most studies, and lack of standardization of treatment methods and comparison groups. A year 2013 systematic review of acupuncture in cancer care included 11 randomized trials in which nausea and vomiting were assessed; eight were considered to have a high risk of bias Only one trial
119
118
.
had a low risk of bias and was positive for short term benefit
of electro acupuncture after chemotherapy for breast cancer. The authors concluded that based upon the single positive study with low risk of bias that acupuncture could be considered an appropriate adjunctive treatment for IV chemotherapy-induced nausea and vomiting but that additional studies were needed. 1.12.3. Other nonpharmacologic strategies Findings from randomized controlled trials of reasonable quality provide limited support for several nonpharmacologic methods to reduce CINV, including cognitive distraction (eg, playing video games during treatment), systematic desensitization (a cognitive approach using visualization and learned relaxation techniques), exercise, hypnosis, acupuncture, and transcutaneous electrical nerve stimulation 120.
55
Chapter two Patients and Methods
Patients & Methods
Patients & Methods
2.1. Study design & settings A randomized single blind controlled clinical trial conducted in Hiwa Teaching Hospital in Sulaimanicity for period from 1st of January to the 31st of December, 2015. 2.2. Population of the study Patients with Hodgkin's lymphoma presented to Hiwa Hospital for Cancer were the study population. 2.3. Medication the first time Aprepitant was supplied by MSD Pharmaceutical as a donation for Hiwa Hospital, while in the second time the drug was donated to Hiwa Hospital by the student. The Placebo was made by the student from Glucose powder. The rescue medication was decided by the Doctor on call when the patient was admitted back to the Hospital.
Inclusion criteria 1. Hodgkin's lymphoma. 2. Patients receiving ABVD chemotherapy regimen which consist of (Adriamycin, Bleomycin,Vinblastine and Dacarbazine). 3. Age between 18-70 years. 4. Patients receiving the first day of the chemotherapy. 57
Patients & Methods Exclusion criteria 1. Patients with another type of tumor or treated with another chemotherapy regimen. 2. Younger than 18 years or older than 70 years. 3. Patients receiving treatment for peptic ulcer 4. Pregnancy. 5. Alcohol intake 6. Patients with severe hepatic impairment. 7. Patients with heart failure. 8. Patients with renal failure. 9. Planned receipt of concomitant stem cell rescue therapy or planned receipt of multiple-day chemotherapy in cycle 1. 10.Radiation therapy to the abdomen or pelvis any time from 1 week before day 1 to day 6. 11.Active infection. 12.Primary or metastatic CNS malignancy. 13.Any uncontrolled disease other than malignancy that the investigator determined might pose an unwarranted risk. 14.Vomiting and/or dry heaves/retching 24 h before chemotherapy.
2.4. Sampling & randomization A total convenient sample of 70 Hodgkin's lymphoma patients presented to Hiwa Center for Cancer and treated with ABVD chemotherapy regimen were selected. Patients received either the treatment(Aprepitant,Ondansetron and Dexamethason) or the standard regimen (Ondansetron, Dexamethason) in a 1:1 ratio according to a computer-generated, random allocation schedule. The selection of both groups was known by the researcher after taking the agreement of Physician responsible of patients' treatment. 58
Patients & Methods 2.5. Treatment protocol Study regimens were administered in a triple-dummy fashion with matching placebos. In the treatment regimen, oral aprepitant was given on days 1–3 (day 1, 125 mg 1 h before chemotherapy; days 2–3, 80 mg); ondansetron was given on day 1 only (day 1, 32 mg i.v. infused over 15 min at 30–60 min prior to chemotherapy; days 2–4, oral placebo twice daily); and oral dexamethasone was given on days 1–4 (day 1, 12 mg 30 min before chemotherapy; days 2–4, 8 mg in the morning and placebo in the evening). In the standard regimen, ondansetron was given on days 1–4 (day 1, 32 mg i.v. infused over 15 min at 30–60 min prior to chemotherapy; days 2–4, 8 mg orally twice daily); and oral dexamethasone was given on days 1–4 (day 1, 20 mg 30 min before chemotherapy; days 2–4, 8 mg twice daily). Because aprepitant has been shown to increase dexamethasone levels approximately two-fold via a CYP3A4 interaction14,15 imp5, the dose of dexamethasone was reduced in the treatment regimen to ensure similar plasma levels between the treatment groups.
59
Patients & Methods
Table 2.1: Treatment Protocol Treatment Group
Aprepitant
Ondansetron
Dexamethason
Day 1
125mg
32mg I.V
12mg
Day 2
80mg
Day 3
80mg
Placebo morning Placebo evening Placebo morning Placebo evening Placebo morning Placebo evening Ondansetron
8mg morning Placebo evening 8mg morning Placebo evening 8mg morning Placebo evening Dexamethason
32mg I.V
20mg
8mg morning 8mg evening 8mg morning 8mg evening 8mg morning 8mg evening
8mg morning 8mg evening 8mg morning 8mg evening 8mg morning 8mg evening
Day 4 Standard Group
Aprepitant
Day 1 Day 2 Day 3 Day 4
60
Patients & Methods
Figure 2.1: Sampling and randomization schedule
2.6. Assessment Quality of life was measured using a validated patient self-assessment FLIE tool. The FLIE consists of nine nausea-specific and nine vomiting-specific items that address the effect of nausea and vomiting on daily functioning following chemotherapy. Responses to each of the 18 items will be marked by the patient with a vertical line on a 100-mm visual analog scale, with anchors being “a great deal” and “none/not at all.” Because optimal antiemetic treatment should eliminate any impact of CINV on QoL, the FLIE endpoint of no impact on daily life (NIDL) will evaluated, NIDL is defined as an item score ≥ 83.3 mm. Patients with No effect are those who had nausea or vomiting average score ≥83.3mm, while patients with Effect are those patients who had nausea or vomiting average score <83.3mm. 61
Patients & Methods FLIE questions Nausea Domain 1. Quantity of nausea. 2. Ability to maintain usual recreation or leisure activities. 3. Ability to make a meal or do minor household repairs. 4. Ability to enjoy a meal. 5. Ability to enjoy liquid refreshment. 6. Willingness to spend time with family/friends. 7. Affected daily functioning. 8. Imposed personal hardship. 9. Imposed hardship on others. Vomiting Domain 1. Quantity of vomiting. 2. Ability to maintain usual recreation or leisure activities. 3. Ability to make a meal or do minor household repairs. 4. Ability to enjoy a meal. 5. Ability to enjoy liquid refreshment. 6. Willingness to spend time with family/friends. 7. Affected daily functioning. 8. Imposed personal hardship. 9. Imposed hardship on others.
2.7. Ethical protocol 1. An approval was obtained from the Ethical Committee from Faculty of Medical Science. 2. A written informed consent was taken from each patient before participation in the study. 3. Rescue medications used when the patient status is deteriorated. 4. Each patient had the right to withdrawal anytime. 62
Patients & Methods 5. Each patient was managed and followed up by a medical team with help of researcher.
Statistical analysis All patients' data entered using computerized statistical software; Statistical Package for Social Sciences (SPSS) version 23 was used. Descriptive statistics presented as (mean ± standard deviation) and frequencies as percentages. Kolmogorov Smirnov analysis verified the normality of the data set. Multiple contingency tables conducted and appropriate statistical tests performed. Chi-square test was used to compare between categorical variables and Independent sample t-test was used to compare between two means. One way ANOVA analysis was used to compare between more than two means. In all statistical analysis, level of significance (p value) set at ≤ 0.05 and the result presented as tables and/or graphs. Statistical analysis of the study was done by the community medicine specialist.
63
Chapter Three Results
Results
Results A total of sixty three Hodgkin's lymphoma patients were included in present study with mean age as 47.8±14.4 years, 34.9% of them were aging 60 years and more. Male patients in present study were more than female with male to female ratio as 1.7:1. All these findings were shown in Table 3.1 and Figures 3.1, 3.2.
Table 3.1: Demographic characteristics of study participants. Variable Age mean±SD (47.8±14.4) years <20 years 20-29 years 30-39 years 40-49 years 50-59 years ≥60 years Total Gender Male Female Total
No.
%
2 5 14 12 8 22 63
3.2 7.9 22.2 19.0 12.7 34.9 100.0
40 23 63
63.5 36.5 100.0
65
Results 25
20
No.
15
10
5
0 <20
20-29
30-39
40-49
50-59
≥60 years
Figure 3.1: Age distribution of study participants.(Years)
36.5% 63.5%
Male Female
Figure3.2: Gender distribution of study participants.
66
Results Mean nausea scores at 1st day of studied patients was 6.5±0.49, 93.7% of patients had no nausea effect. Mean nausea scores at second day was 5.3±0.75, 20.6% of patients had no nausea effect. Mean nausea scores of studied patients at third day was 5.3±0.8, 25.4% of them had no nausea effect and mean nausea scores of the patients at 4th day was 6.3±0.79, 73% of them had no nausea effect. The mean total nausea scores of Hodgkin's lymphoma patients was 5.8±0.6, 46% of them had no nausea effect. All these findings were shown in Table 3.2 and Figure 3.3. Table 3.2: Nausea scores and nausea effect of study participants. Variable
No.
Nausea scores at 1st day mean±SD (6.5±0.49) No effect 59 Effect 4 Total 63 Nausea scores at 2nd day mean±SD (5.3±0.75) No effect 13 19.0 Effect 50 Total 63 Nausea scores at 3rdday mean±SD (5.3±0.8) No effect 16 Effect 47 Total 63 Nausea scores at 4th day mean±SD (6.3±0.79) No effect 46 Effect 17 Total 63 Total nausea scores mean±SD (5.8±0.6) No effect 29 Effect 34 Total 63
67
% 93.7 6.3 100.0 20.6 79.4 100.0 25.4 74.6 100.0 73.0 27.0 100.0 46.0 54.0 100.0
Results Mean vomiting scores at 1st day of studied patients was 6.7±0.4, 96.8% of patients had no emesis effect. Mean vomiting scores at second day was 5.7±0.7, 52.4% of patients had no emesis effect. Mean vomiting scores of studied patients at third day was 5.7±0.8, 47.6% of then had no emesis effect and mean vomiting scores of the patients at 4th day was 6.1±0.79, 73% of them had no emesis effect. The mean total vomiting scores of Hodgkin's lymphoma patients was 6.0±0.6, 61.9% of them had no emesis effect. All these findings were shown in Table 3.3 and Figure 3.3. Table 3.3: Vomiting scores and emetic effect of study participants. Variable
No.
Vomiting scores at 1st day mean±SD (6.7±0.4) No effect 61 Effect 2 Total 63 Vomiting scores at 2nd day mean±SD (5.7±0.7) No effect 33 19.0 Effect 30 Total 63 Vomiting scores at 3rd day mean±SD (5.7±0.8) No effect 30 Effect 33 Total 63 Vomiting scores at 4th day mean±SD (6.1±0.79) No effect 46 Effect 17 Total 63 Total vomiting scores mean±SD (6.0±0.6) No effect 39 Effect 24 Total 63
68
% 96.8 3.2 100.0 52.4 47.6 100.0 47.6 52.4 100.0 73.0 27.0 100.0 61.9 38.1 100.0
Results 45 40 35
No.
30 25
No effect
20
Effect
15 10 5 0 Nausea
Vomiting
Figure 3.3: Total emesis effect of all study patients. Only 7 (11.1%) patients needed rescue medications, Figure 3.4.
7 (11.1%)
Need 56(88.9%)
Not need
Figure 3.4: Distribution of rescue medications.
69
Results No significant differences were observed between treatment and standard groups regarding age and gender (p>0.05). There was a significant association between needing to rescue medications and standard group patients (p=0.02). All these findings were shown in Table 3.4 and Figure 3.5.
Table 3.4: Distribution of demographic characteristics and rescue medications of study participants according to study groups. Variable
Treatment group No. %
Age <20 years 1 20-29 years 1 30-39 years 10 40-49 years 8 50-59 years 4 ≥60 years 11 Gender Male 22 Female 13 Rescue medications Need 0 Not need 35 *Fishers exact test.
2.9 2.9 28.6 22.9 11.4 31.4 62.9 37.1 100.0
Standard group No. % 1 4 3 4 5 11 18 10 7 21
70
χ²
P
6.3*
0.2
0.01
0.9
9.8*
0.02
3.6 14.3 10.7 14.3 17.9 39.3 64.3 35.7 25.0 75.0
Results 40 35 30
No.
25 Need rescue
20
Not need resue
15 10 5 0 Treatment
Standard
Figure 3.5: Distribution of rescue medications according to study groups.
As shown in Table 3.5 and Figure 3.6 and according to nausea scores, no significant difference was observed between treatment and standard groups patients regarding nausea effect at first day (p=0.06). There was a significantly higher nausea effect among standard group patients at second day (p=0.003). No nausea effect was significantly higher among treatment group patients than standard group at 3rd day (p=0.003). A significant higher no nausea effect was observed among treatment group patients at the fourth day (p=0.002). There was a highly significant association between total no nausea effect and treatment group patients (p<0.001).
71
Results Table 3.5: Distribution of nausea scores and nausea effect of study participants according to study groups. Variable
Treatment group No. % Nausea scores at 1st day No effect 31 88.6 Effect 4 11.4 Nausea scores at 2nd day No effect 12 34.3 Effect 23 65.7 Nausea scores at 3rd day No effect 14 40.0 Effect 21 60.0 th Nausea scores at 4 day No effect 31 88.6 Effect 4 11.4 Total nausea scores No effect 23 65.7 Effect 12 34.3
Standard group No. % 28 0 1 27 2 26 15 13 6 22
χ²
P
3.4*
0.06
8.9
0.003
8.8
0.003
9.6
0.002
12.2
<0.001
100.0 3.6 96.4 7.1 92.9 53.6 46.4 21.4 78.6
25
20
15
No.
No effect Effect
10
5
0 Treatment
Standard
Figure 3.6: Distribution of nausea score and emesis effect according to study groups. 72
Results
As shown in Table 3.6 and Figure 3.7 and according to vomiting scores, no significant difference was observed between treatment and standard groups patients regarding emesis effect at first day and second day (p>0.05). No emesis effect was significantly higher among treatment group patients than standard group at 3rd day (p<0.001). A significant higher no emesis effect was observed among treatment group patients at the fourth day (p=0.002). There was a highly significant association between total no emesis effect and treatment group patients (p=0.005).
Table 3.6: Distribution of vomiting scores and emetic effect of study participants according to study groups. Variable
Treatment group No. % Vomiting scores at 1st day No effect 33 94.3 Effect 2 5.7 Vomiting scores at 2nd day No effect 22 62.9 Effect 13 37.1 rd Vomiting scores at 3 day No effect 25 71.4 Effect 10 28.6 th Vomiting scores at 4 day No effect 31 88.6 Effect 4 11.4 Total vomiting scores No effect 27 77.1 Effect 8 22.9
Standard group No. % 28 0 11 17 5 23 15 13 12 16
73
χ²
P
1.6*
0.1
3.4
0.06
17.8
<0.001
9.6
0.002
7.7
0.005
100.0 39.3 60.7 17.9 82.1 53.6 46.4 42.9 57.1
Results
30 25 20
No.
No effect 15
Effect
10 5 0 Treatment
Standard
Figure 3.7: Distribution of vomiting score emesis effect according to study groups.
As shown in Table 3.7 and Figure 3.8, there was no significant difference between two study groups in mean nausea scores at first day (p=0.3). A significant higher mean nausea scores was observed for treatment groups patients at 2nd, 3rdand 4thdays than standard group patients (p<0.05). There was a significant higher total mean nausea scores for treatment group patients (p=0.001).
Table 3.7: Distribution of nausea scores of study participants according to study groups. Nausea Scores 1st day 2nd day 3rdday 4th day Total
Treatment Mean±SD 6.5±0.5 5.6±0.7 5.5±0.8 6.4±0.49 6±0.5
Standard Mean±SD 6.6±0.4 5±0.69 4.9±0.6 5.6±0.8 5.5±0.5
74
t-test
P
1.0 3.3 3.4 5.03 3.4
0.3 0.001 0.001 <0.001 0.001
Results 6.5
Mean score
6
5.5
2nd day 3rd day 4th day
5
Total 4.5
4 Treatment
Standard
Figure 3.8: Distribution of nausea scores according to study groups. As shown in Table 3.8 and Figure 3.9, there was significant higher mean vomiting scores for treatment groups patients at 2nd , 3rd and 4th days than standard group patients (p<0.05). A significant higher vomiting score was observed among standard group patients than treatment group (p=0.04). There was a highly significant increased total mean vomiting scores for treatment group patients (p<0.001). Table 3.8: Distribution of vomiting scores of study participants according to study groups. Vomiting Scores 1st day 2nd day 3rdday 4th day Total
Treatment Mean±SD 6.4±0.4 6±0.6 6.1±0.59 6.4±0.49 6.3±0.48
Standard Mean±SD 6.8±0.2 5.3±0.7 5.2±0.79 5.6±0.8 5.7±0.5
75
t-test
P
2 4.2 5.2 5.03 4.3
0.04 <0.001 <0.001 <0.001 <0.001
Results
Mean scores
6.5
1st day
6
2nd day 3rd day 5.5
4th day Total
5
4.5 Treatment
Standard
Figure 4.9: Distribution of vomiting scores according to study groups.
There was a significant higher total nausea and vomiting scores for treatment group patients at 1st day (p<0.001). Lowest nausea score of treatment group patients was significantly at 3rd day (p<0.001) and lowest vomiting score of treatment group patients was at 2nd day (p<0.001). All these findings were shown in Table 3.9 and Figure 3.10.
Table 3.9: Distribution of nausea and vomiting scores of treatment group according to administration days. Days First Second Third Fourth ANOVA (P value)
Nausea scores Mean±SD 6.5±0.5 5.6±0.7 5.5±0.8 6.4±0.4 <0.001
76
Vomiting scores Mean±SD 6.6±0.4 6±0.6 6.1±0.5 6.4±0.4 <0.001
Results 6.8 6.6
Mean score
6.4 6.2 Nausea
6
Vomiting
5.8 5.6 5.4 5.2 First
Second
Third
Fourth
Figure 3.10: Distribution of total nausea and vomiting scores according to days of administration.
As shown in Table 3.10, there was a significant higher nausea and vomiting scores for treatment group patients aging less than 40 years than standard group patients aging less than 40 (p<0.001). Table 3.10: Distribution of total nausea and vomiting scores of study participants aging less than 40 years according to study groups. Scores Total nausea Total vomiting
Treatment Mean±SD 6.2±0.3 6.4±0.3
Standard Mean±SD 5.1±0.4 5.5±0.5
77
t-test
P
5.4 4.7
<0.001 <0.001
Results As shown in Table 3.11, no significant difference was observed between treatment group and standard group patients aging 40 years and more regarding nausea scores (p=0.1. There was a significant higher vomiting scores for treatment group patients aging 40 years and more than standard group patients 40years and more (p=0.02).
Table 3.11: Distribution of total nausea and vomiting scores of study participants aging 40 years and more according to study groups. Scores Total nausea Total vomiting
Treatment Mean±SD 5.9±0.6 6.2±0.5
Standard Mean±SD 5.7±0.5 5.8±0.5
t-test
P
1.3 2.4
0.1 0.02
As shown in Table 3.12, there was a significant higher nausea and vomiting scores for male treatment group patients than male standard group patients (p<0.05).
Table 3.12: Distribution of total nausea and vomiting scores of male study participants according to study groups. Scores Total nausea Total vomiting
Treatment Mean±SD 6.1±0.5 6.3±0.4
Standard Mean±SD 5.7±0.4 5.9±0.4
78
t-test
P
2.4 2.8
0.01 0.007
Results As shown in Table 3.13, there was a significant higher vomiting scores for female treatment group patients than female standard group patients (p<0.05).
Table 3.13: Distribution of total nausea and vomiting scores of female study participants according to study groups. Scores Total nausea Total vomiting
Treatment Mean±SD 5.9±0.6 6.3±0.6
Standard Mean±SD 5.2±0.5 5.3±0.6
79
t-test
P
2.6 3.6
0.01 0.001
Chapter Four Discussion
Discussion
Discussion
Nausea and vomiting have long been acknowledged to be among the most feared and distressing side effects of chemotherapy. Chemo- therapy-induced nausea and vomiting (CINV) can have significant effects on both quality of life and physical functioning; in severe cases, CINV can lead to serious complications or a clinical decision to delay, reduce, or even stop chemotherapy
121
. As a consequence, control of CINV is a high priority for
improving clinical outcomes in patients with cancer48.Cisplatin is the main example of a drug with a high emetogenic potential; doses greater than 50mg/m2lead to nausea and vomiting in more than 90% of patients if no prophylactic therapy is used. Other drugs with high emetogenic potential include cyclohosphamide (>1,500 mg/m2), carmustine (>250 mg/m2), and dacarbazine122. 4.1. Demographic characteristics 4.1.2. Age In this study the mean age of was 47.8±14.4 years; about two thirds of studied patients were in middle age group. These findings are not similar to results of retrospective study conducted in Sulaimani
123
that reported median age of
Hodjkins lymphoma patients as 31 years. The incidence of Hodgkin's lymphoma has increased among adolescents and young adults in the Nordic countries in the past few decades, whereas it has decreased strikingly among those aged 40 years or more
124
. In developing
countries, Hodgkin's lymphoma appears more during childhood and its 81
Discussion incidence decreases with age, while in developed countries, young children are rarely affected by Hodgkin's lymphoma in contrast with young adults where incidence increase with age
125
. It has a bimodal age distribution in both sexes,
peaking in young adults (aged 15-34 y) and older individuals (>55years)
125
. In
the United States, Nodular sclerosing subtype predominates in young adults, while mixed cellularity subtype is more common in children (aged 0-14 y) and older individuals126. From 2004-2008, the median age at diagnosis for Hodgkin's lymphoma was 38 years of age and approximately 12.3% were diagnosed under age 20 years and 27.7% above 55 years of age124. There are two peaks in the age-specific incidence of Hodgkin's lymphoma. For males there is one in men aged 30-34 and another in older men aged 75-79 years. For women the two peaks occur in women aged 20-24 and 70-79
127
.
Hodgkin's lymphoma is the third most common cancer in people aged 15-29 years, and the sixth most commonly diagnosed cancer in children less than 14 years 128. 4.1.2. Gender In current study, male patients with Hodgkin's lymphoma were more than females. This is consistent with Smith et al
129
study in UK which reported that
males tended to be diagnosed at younger ages and have significantly (P<0.05) higher incidence rates. Differences were greatest at younger ages: the <15 year male/female rate ratio for all subtypes combined being 2.2 (95% CI 1.3–3.4). These gender differences impacted on prevalence; most subtype estimates being significantly (P<0.05) higher in males than females. Outcome varied widely by subtype; survival of patients with nodular lymphocyte predominant Hodgkin lymphoma approached that of the general population, whereas less than a third of those with other B-cell (e.g., mantle cell) or T-cell (e.g., peripheral-T) lymphomas survived for >5 years. No males/female survival differences were detected129.
82
Discussion In adolescents, the incidence between males and females are roughly equal. Data from Norway showed that a sex ratio of 1:1 is seen in the 15-34 age groups which increase to 2:1 in the 50 and over group126. Hodgkin's lymphoma is nearly twice as common in males. It is higher in males than females and higher in whites than other races
130
. Men are affected by Hodgkin's lymphoma
slightly more than women among all subtypes except for the nodular sclerozing subtype. The observed male predominance is particularly evident in children, in whom 85% of the cases are in males125. Males consistently tending to have significantly higher age-standardized incidence rates and to be diagnosed at younger ages, resulting in a doubling of the male/ female rate ratio for all lymphomas combined in those diagnosed before 15 years of age. Such strong gender differences have a big impact on prevalence; the combined lymphoma 10-year prevalence estimate in our data set being 30 per 100 000 higher in males than in females. That hematological malignancies often occur more frequently in males than females has been noted by others 131; and in this regard subtypes that fail to exhibit these incidence/age features stand out; follicular lymphoma being the only mature B-cell lymphoma to occur significantly more frequently in women than men and nodular sclerosis classical Hodgkin lymphoma being the only one with a significantly younger diagnostic age in females than males129. Our study found no significant differences between two study groups regarding age and gender. This is consistent with results of American clinical trial study which evaluated Aprepitant role in two carcinoma patient groups and revealed no significant differences in age and gender.imp3 This finding increased the validity and power of the study. 4.2. Nausea score 4.2.1. Acute phase Present study found no significant difference between treatment group Hodgkin's lymphoma patients treated with (Aprepitant,Ondansetron and 83
Discussion Dexamethasone)
and
standard
group
treated
with
(Ondansetron,
Dexamethasone).This finding is in agreement with results of Ng et al
132
study
in England which concluded that Ondansetron and Dexamethasone regimen did not adequately control acute nausea of patients with carcinoma. This finding is inconsistent with Aziz study in USA
133
which stated that NK1R antagonists
improved control of CINV in the acute, delayed, and overall phases for patients who received highly and moderately emetogenic chemotherapy. CINV control in the acute phase seemed to be a surrogate for CINV control in the delayed phase. Early clinical data demonstrated that aprepitant represented a new class of antiemetic therapy, with an efficacy profile distinct from those of 5HT3 RAs or dexamethasone, providing enhanced control of both acute and delayed CINV when co-administered with a 5HT3 RA and dexamethasone compared with dual therapy alone 134, 135. An initial study showed that the triple combination of aprepitant, granisetron, and dexamethasone was statistically better than granisetron and dexamethasone for preventing cisplatin-related acute and delayed CINV, supporting further study of triple therapy 70. Furthermore, in a small, randomized, proof-of-concept trial, fosaprepitant was superior to ondansetron in preventing delayed CINV when each was administered as a single agent, supporting the combination of fosaprepitant with a 5HT3 RA and dexamethasone
134
. Early studies also determined the most effective dose of
aprepitant when combined with standard antiemetic regimens for prevention of CINV, adjusting for the pharmacokinetic interaction of aprepitant and dexamethasone 136. Our findings regarding weak effect of (Aprepitant,Ondansitron and Dexamethasone) regimen at acute phase are similar to results of Hesketh et al 20 study in USA which reported overall significant effect of aprepitant when added to ondansitron and dexamethasone in suppressing CINV but week antiemetic effect was documented in first day. 84
Discussion NK1R antagonists are known to increase the bioavailability of dexamethasone, and this pharmacokinetic interaction could potentially play a role in the higher incidence of infection among patients who have been treated with NK1R antagonists133. The Chawla et al
137
study did not decrease the day 1
dexamethasone dose in the NK1R arm, whereas the Schmoll et al138 and PoliBigelli et al139 studies did. Nevertheless, it seems unlikely that increased dexamethasone bioavailability could have any impact on the infection rates because these three trials presented similar findings. NK1R antagonists can also increase the bioavailability of chemotherapy agents metabolized by cytochrome P450 3A4 (CYP3A4), such as etoposide, taxanes, irinotecan, vinca alkaloids, anthracyclines, and cyclophosphamide. Two of three studies suggested that adverse events could be more common among patients receiving an NK1R antagonist plus a CYP3A4-metabolized chemotherapy 140. Nausea occurred in fewer patients in the aprepitant group, but the results were not significantly different from those in the control group. This result is in line with other aprepitant studies in which patients received either highly or moderately emetogenic chemotherapy, which suggests that the neurokinin-1 receptor antagonists may have less impact on the nausea component of chemotherapy-induced nausea and vomiting. In general, the control of nausea lags behind the control of vomiting, perhaps because of the difficulty of measuring this subjective symptom and the possibility that patients confuse nausea with anorexia, fatigue or pyrosis 138. 4.2.2. Delayed phase Current study revealed that delayed nausea score for patients taking treatment (Aprepitant,Ondansetron and Dexamethasone) regimen was significantly higher than those taking standard regimen. In other word, nausea effects were significantly decreased among patients taking treatment regimen in comparison to patients taking standard regimen. These findings are consistent with results of Schmitt et al
105
study in USA which found that addition of aprepitant 85
Discussion resulted in significantly less CINV and had a positive effect on quality of life. Aoki et al 5 study in Japan which retrospectively investigated the rates of emetic control by a combination of granisetron, 5-HT antagonist and dexamethasone in various HEC regimens, including 5 single-day chemotherapy regimens such as
gemcitabine/cisplatin
(GEM/CDDP),
epirubicin/cyclophosphamide
(EPI/CPA), pemetrexed or vinorelbine/cisplatin (PEM or VNR/CDDP), doxorubicin/bleomycin/ rituximab/doxorubicin/ CHOP21), and
vinblastine/dacarbazine
(ABVd)
cyclophosphamide/vincristine/prendisolone
and (R-
2 multiple-day chemotherapy regimens such as 5-
fluorouracil/cisplatin (5-FU/CDDP) and bleomycin/etoposide/ cisplatin (BEP). Complete response (no emesis, no rescue treatment) during the overall period (days 1-5) was assessed as the primary endpoint. Chemotherapy-induced nausea and vomiting was well-controlled (complete response >70%) in GEM/CDDP and R-CHOP21, but not in other regimens. The effect of a triple antiemetic medication including aprepitant (APR) was subsequently examined in patients receiving EPI/CPA and 5-FU/CDDP. Complete response was significantly improved in patients receiving 5-FU/CDDP but not in those receiving EPI/CPA, although the complete protection from vomiting significantly increased in both cases. Of note, the administration of APR for 5 days, but not for 3 days, was required to completely block the incidence of vomiting during the 7 days of the observation period in patients receiving 5FU/CDDP. These findings suggest that APR should be used appropriately based on the emetogenicity of HEC regimens5. The important advances in preventive therapy for CINV have been the approval of the neurokinin-1 (NK1) receptor antagonist aprepitant. In 2 large trials including> 1000 patients, aprepitant substantially improved antiemetic protection when combined with a standard regimen of a 5HT3 antagonist plus a
86
Discussion corticosteroid, particularly in the 2–5 days after chemotherapy (delayed phase)139, 141.
4.3. Vomiting score 4.3.1. Acute phase Vomiting
scores
for
cancer
patients
on
treatment
regimen
(Aprepitant,Ondansetron and Dexamethasone) were significantly higher than vomiting scores reported for cancer patients on standard regimen Ondansetron, Dexamethasone) (p=0.04). This is similar to results of Schmoll et al
138
study in
USA which reported that in comparison an antiemetic regimen in which ondansetron + dexamethasone were given for 4 days, the aprepitant regimen was superior in the acute, delayed and overall phases of chemotherapy-induced nausea and vomiting. In this study, the aprepitant regimen was superior to the control regimen (ondansetron plus dexamethasone both given for 4 days) in providing complete response, primarily because of excellent efficacy in preventing vomiting. Complete response rates were higher in the aprepitant group for the overall phase (0–120 h post-cisplatin), as well as in separate assessments of the acute and delayed phases. As in previous studies, the between-group difference in the complete response rate was more pronounced in the delayed phase than in the acute phase. Acute-phase vomiting after cisplatin treatment is thought to be primarily mediated via the serotonin receptors, the site of action of 5-HT3 RAs. The mechanism for post-cisplatin delayed-phase vomiting is not well understood, but the generally lower efficacy of 5-HT3 receptor antagonists in the delayed phase points to a lesser role for serotonin. Another supporting line of evidence for a non-serotonin mechanism comes from the finding that the urinary level of the serotonin metabolite 5-hydroxyindoleacetic acid, which reflects gastrointestinal serotonin release and turnover, increases in association 87
Discussion with cisplatin-induced acute-phase vomiting, but returns to baseline levels during delayed-phase vomiting 142. Another analysis of the time course of the antiemetic effect of 5-HT3 receptor antagonists and the NK1 receptor antagonist aprepitant indicated that while serotonin-dependent mechanisms predominate in the acute phase, NK-1dependent mechanisms predominate in delayed-phase vomiting 143. Patients in the aprepitant group also had a longer duration of protection against the first vomiting episode that observed in other studies which compared an aprepitant regimen and various multiple-day ondansetron-based control regimens in patients receiving highly emetogenic chemotherapy
141
and in
breast cancer patients receiving moderately emetogenic chemotherapy 73. 4.3.2.Delayed phase Vomiting scores with delayed effect for patients taking treatment regimen as acute phase were significantly higher than vomiting scores for patients taking standard regimen. These findings are consistent with results of Poll-Bigelli et al 141
study in Brazil which concluded that apprepitant regimen had superior effect
in suppressing delayed vomiting effect for cancer patients on chemotherapy. Whereas acute vomiting is known to depend primarily on serotonin, the pathophysiology of delayed vomiting is less well understood and multiple mechanisms may contribute 144. Neurokinin-1 (NK) receptors are found in brain regions critical to regulating the vomiting reflex and a recent analysis of studies suggested a possible predominance of NK1-related mechanisms during delayed-phase vomiting 143. Aprepitant is a selective, high affinity NK receptor antagonist. In patients receiving highly emetogenic chemotherapy, a regimen combining aprepitant with ondansetron plus dexamethasone on day 1, before chemotherapy, improved complete response rates by 11–14 percentage points in the acute phase and aprepitant plus dexamethasone improved complete response rates by 20 percentage points in the delayed phase 139, 141.
88
Discussion
4.4. Rescue medications The need for rescue medications was significantly constrained only among patients taking standard regimen (p=0.02). This finding is in agreement with results of Yeo et al
145
study in China which reported that use of aprepitant
regimen reduces the requirement of rescue medications when compared to control regimen for prevention of CINV in patients receiving chemotherapy and is associated with better quality of life. Hu et al
146
study in South Korea
which was a prospective study on patients with lung cancer and investigating the role of aprepitant among those patients found that no patients on aprepitant regimen needed recue medications.
Limitations of the study 1. Single center study that cannot be generalized on Iraqi population. 2. Loss to follow up.
89
Chapter Five Conclusions & Recommendations
Conclusions & Recommendations
Conclusions
The use of Aprepitant,Odansetron and Dexamethasone regimen showed superior and valuable results in prevention of cancer induced nausea and vomiting by patients on chemotherapy. Aprepitant,Odansetron and Dexamethasone regimen had good delayed effect in suppressing nausea induced by chemotherapy. Aprepitant,Odansetron and Dexamethasone regimen had good acute and delayed effect in suppressing vomiting induced by chemotherapy. Aprepitant,Odansetron and Dexamethasone regimen prevent the need to rescue medications.
91
Conclusions & Recommendations
Recommendations
Implementation of aprepitant regimen for all cancer patients treated with highly emitogenic chemotherapy in all Iraqi centers. Encourage the availability of aprepitant and 5HT3 therapy by the government and other agencies to alleviate the patient's sufferings. Another national wide size studies on aprepitant regimens effect should be supported.
92
References
References
References 1. Yeh CH, Chin LC, Chiang YC, Lin SW, Huang CK, Ren D. Reduction in nausea and vomiting in adolescents undergoing cancer chemotherapy by either appropriate or sham auricular acupuncture points with standard care. The Journal of Alternative and Complementary Medicine. 2012; 18(4): 334-40. PMId:22515794 http://dx.doi.org/10.1089/a 2. Newton S, Hickey M, Marrs J. Oncology nursing advisore. Ohio: Mosby Elsevier Co; 2009. 100 p. 3. Hasanen
AE. Side-Effect
management technique for
leukemic
adolescents undergoing chemotherapy. Unpublished Thesis for Doctorate degree. Faculty of Nursing Mansoura University. 2014. 4. Lebaron S, Zeltzer LK, Lebaron C, Scott SE, Zelter PM. Chemotherapy side effects in pediatric oncology patients: Drugs, age, and sex as risk factors. Medical and Pediatric Oncology. 2008; 16(4): 263-268. http://dx.doi.org/10.1002/mpo.2950160408 5. Aoki S, Iihara H, Nishigaki M, Imanishi Y, Yamauchi K, Ishihara M, et al. Difference in the emetic control among highly emetogenic chemotherapy regimens: Implementation for appropriate use of aprepitant. Molecular and Clinical Oncology. 2013; 1(1):41-46. 6. Carpenter DO. Central nervous system mechanisms in deglutition and emesis. ComprPhysiol 2011, Supplement 16: Handbook of Physiology, The Gastrointestinal System, Motility and Circulation: 685-714. 7. Teunissen SC, Wesker W, Kruitwagen C, DeHaes HC, Voest EE, Graeff A. Symptom prevalence in patients with incurable cancer: a systematic review. J Pain Symptom Manage 2007; 34(1):94–104.
94
References 8. Sankhala K, Pandya D, Sarantopoulos J, Soefje S, Giles F, Chawla S. Prevention of chemotherapy induced nausea and vomiting: a focus on aprepitant. Expert Opinion on Drug Metabolism & Toxicology 2009; 5(12):1607-1614. 9. Emend (aprepitant capsules). Prescribing information. Whitehouse Station, NJ: Merck & Co. Inc.: March 2003. Available at: http://www.fda.gov/cder/foi/label/2003/21549_Emend_lbl.pdf. 10.Am J Health Syst Pharm: Therapeutic Guidelines on the Pharmacologic Management of Nausea and Vomiting in Adult and Pediatric Patients Receiving Chemotherapy or Radiation Therapy or Undergoing Surgery. 1999; 56:729–764. 11.Ballatori E, Roila F. Impact of Nausea and Vomiting on Quality of Life in Cancer Patients during Chemotherapy. Health and Quality of Life Outcomes 2003; 1:46. 12.Eisenberg P, Figueroa-Vadillo J, Zamora R, Charu V, Hajdenberg J, Cartmell A, et al. Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer 2003; 98(11):2473-2482. 13.Basch E, Prestrud AA, Hesketh PJ. Antiemetics: American society of clinical oncology: Clinical practice guidelines update ASCO 2011 Guidelines 14.Schwartzberg L, Jackson J, Jain G, et al. Impact of 5-HT RA selection within triple antiemetic regimens on uncontrolled highly emetogenic chemotherapy-induced nausea/vomiting. Expert Rev Pharmacoecon Outcomes Res. 2011; 11:481-488.
95
References 15.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): antiemesis. Version 2.2014.www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf. 16.Billio A, Morello E, Clarke MJ. Serotonin receptor antagonists for highly emetogenic chemotherapy in adults. Cochrane Database Syst Rev.Jan 2010:CD006272. Update in: Cochrane Database Syst Rev. 2013; 12:CD006272. 17.Feinberg B, Gilmore J, Haislip S, Jackson J, Jain G, Balu S, et al. Impact of
initiating
antiemetic
prophylaxis
with
palonosetron
versus
ondansetron on risk of uncontrolled chemotherapy-induced nausea and vomiting in patients with lung cancer receiving multi-day chemotherapy. Support Care Cancer 2012; 20:615-623. 18.Basch E, Prestrud AA, Hesketh PJ, et al; for the American Society of Clinical Oncology. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J ClinOncol 2011; 29:4189-4198. 19.Grunberg S, Chua D, Maru A, Dinis J, DeVandry S, Boice JA, et al. Single-dose fosaprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with cisplatin therapy: randomized, double-blind study protocol - EASE. J ClinOncol2011; 29: 1495-1501. 20.Hesketh PJ, Grunberg SM, Herrstedt J, de Wit R, Gralla RJ, Carides AD, et al. Combined data from two phase III trials of the NK1 antagonist aprepitant plus a 5HT antagonist and a corticosteroid for prevention of chemotherapyinduced nausea and vomiting: effect of gender on treatment response. Support Care Cancer 2006; 14: 354-360. 21.World Health Organization. Cancer Control Program. WHO 2012. Available on: http://www.who.int/cancer/en/ 22.American Cancer Society. The History of Cancer. 2011. Available on: www.cancer.org/acs/groups/cid/documents/.../002048-pdf.pdf 96
References 23.Davies A, Epstein JD. Oral complications of cancer and its management. Oxford: Oxford University Press 2010. 24.Spreadbourgh D, Read J. Radiotherapy. In M. GRUNDY (2nd Ed.), Nursing in Haematological Oncology. Edinburgh: Bailliere Tindall; 2000.164. 25.Peterson DE, Lalla R. Overview of complications of systematic chemotherapy. In Davies A, Epstein JB (1st Eds.), Oral complications of cancer and its management. Great Britain: Oxford University Press 2010.3. 26.Castello BA, Erlichman C. Survivorship. In Chabner BA, Longo DL , Cancer Chemotherapy and Biotherapy: Principles and Practice (Fifth ed.): Lippincott Williams & Wilkin 2010.55 27.Abu-SaadHuijer H, Abboud S, Doumit M. Symptom Prevalence and Management of Cancer Patients in Lebanon. Journal of Pain and Symptom Management2012; 44(3): 386-399. 28.Horn CC. Why is the neurobiology of nausea and vomiting so important? Appetite 2008; 50(2-3): 430-434. 29.Tadman M, Roberts D. Oxford Handbook of Cancer Nursing (1 sted.). New York: Oxford University Press 2007. 30.Harbord M. Nausea and vomiting. Medicine 2009; 37(2):115-118. 31.Baker PD, Morzorati SL, Ellett ML. The Pathophysiology of Chemotherapy-Induced Nausea and Vomiting. Gastroenterology Nursing 2005; 28(6): 469-480. 32.Middleton J, Lennan E. Effectively managing chemotherapy induced nausea and vomiting. British Journal of Nursing 2011; 20(17): s7-s15. 33.Dewan P, Singhal S, Harit D. Management of Chemotherapy-Induced Nausea and Vomiting. Indian Pediatrics 2010; 47(2): 149-155.
97
References 34.Schwartzberg
L.
Chemotherapy-Induced
Nausea
and
Vomiting:
Clinician and Patient Perspectives. The Journal of Supportive Oncology 2007; 5(2): 5-13. 35.Aapro MS, Molassiotis A, Olver I. Anticipatory nausea and vomiting. Support Care Cancer 2005; 13: 117-121. 36.Hesketh PJ. Chemotherapy-Induced Nausea and Vomiting. The New England Journal of Medicine 2008; 358(23): 2482-2494. 37.Feyer P, Jordan K. Update and new trends in antiemetic therapy: the continuing need for novel therapies. Ann Oncol 2011; 22:30–38. 38.Hilarius DL, Kloeg PH, van der Wall E. Chemotherapy-induced nausea and vomiting in daily clinical practice: a community hospital-based study. Support Care Cancer 2012; 20:107–117. 39.Grunberg SM, Deuson RR, Mavros P. Incidence of chemotherapyinduced nausea and emesis after modern antiemetics. Cancer 2004; 100:2261–2268. 40.Decker GM, DeMeyer ES, Kisko DL. Measuring the maintenance of daily life activities using the functional living index-emesis (FLIE) in patients receiving moderately emetogenic chemotherapy. J Support Oncol 2006; 4: 35–41. 41.Beckwith M, Mullin S. Prevention and management of chemotherapyinduced nausea and vomiting, part 1. Hospital Pharmacist 2001; 36:67– 82. 42.Bloechl-Daum B, Deuson RR, Mavros P, Hansen M, Herrstedt J. Delayed nausea and vomiting continue to reduce patients’ quality of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J ClinOncol 2006; 24:4472–4478.
98
References 43.Haiderali A, Menditto L, Good M. Impact on daily functioning and indirect/direct costs associated with chemotherapy-induced nausea and vomiting (CINV) in a U.S. population. Support Care Cancer 2011; 19:843–851. 44.Ihbe-Heffinger A, Ehlken B, Bernard R. The impact of delayed chemotherapy-induced nausea and vomiting on patients, health resource utilization and costs in German cancer centers. Ann Oncol 2004; 15:526– 536. 45.Roila F, Herrstedt J, Aapro M. Guideline update for MASCC and ESMO in the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting: results of the Perugia consensus conference. Ann Oncol 2010; 21 (5):232-243. 46.Basch E, Prestrud AA, Hesketh PJ. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J ClinOncol 2011; 29:4189–4198. 47.Likun Z, Xiang J, Yi B. A systematic review and meta-analysis of intravenous palonosetron in the prevention of chemotherapy-induced nausea and vomiting in adults. Oncologist 2011; 16:207–216. 48.Boccia RV, Gordan LN, Clark G. Efficacy and tolerability of transdermal granisetron for the control of chemotherapy-induced nausea and vomiting associated with moderately and highly emetogenic multiday chemotherapy: a randomized, double-blind, phase III study. Support Care Cancer 2011; 19:1609–1617. 49.Frame DG. Best practice management of CINV in oncology patients: I. Physiology and treatment of CINV. Multiple neurotransmitters and receptors and the need for combination therapeutic approaches. J Support Oncol 2010; 8:5–9. 99
References 50.Jordan K, Sippel C, Schmoll HJ. Guidelines for antiemetic treatment of chemotherapy-induced nausea and vomiting: past, present, and future recommendations. Oncologist 2007; 12:1143–50. 51.Wong H, Tejani A. Neurokinin-1 receptor antagonists for prevention of chemotherapy-related nausea and vomiting in adults–Protocol. Cochrane Database Syst Rev 2012; CD006844. 52.Roila F, Herrstedt J, Aapro M. Guideline update for MASCC and ESMO in the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting: results of the Perugia consensus conference. Ann Oncol 2010; 21 Suppl 5:v232. 53.Basch E, Prestrud AA, Hesketh PJ, Kris MG, Feyer PC, Somerfield MR, et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J ClinOncol 2011; 29:4189. 54.Hesketh PJ, Bohlke K, Lyman GH, Morrow J, Rao KV, Chesney M ,et al. Antiemetics: American Society of Clinical Oncology Focused Guideline Update. J ClinOncol 2015. 55.Chevallier B, Cappelaere P, Splinter T. A double-blind, multicentre comparison of intravenous dolasetronmesilate and metoclopramide in the prevention of nausea and vomiting in cancer patients receiving high-dose cisplatin chemotherapy. Support Care Cancer 1997; 5:22. 56.Davidson N, Rapoport B, Erikstein B, Esperance B, Ruff P, Paska W, et al. Comparison of an orally disintegrating ondansetron tablet with the conventional ondansetron tablet for cyclophosphamide-induced emesis in cancer patients: a multicenter, double-masked study. Ondansetron Orally Disintegrating Tablet Emesis Study Group. ClinTher 1999; 21:492. 57.del Giglio A, Soares HP, Caparroz C, Castro PC. Granisetron is equivalent to ondansetron for prophylaxis of chemotherapy-induced 100
References nausea and vomiting: results of a meta-analysis of randomized controlled trials. Cancer 2000; 89:2301. 58.Gandara DR, Roila F, Warr D. Consensus proposal for 5HT3 antagonists in the prevention of acute emesis related to highly emetogenic chemotherapy. Dose, schedule, and route of administration. Support Care Cancer 1998; 6:237. 59.Kaizer L, Warr D, Hoskins P. Effect of schedule and maintenance on the antiemetic efficacy of ondansetron combined with dexamethasone in acute and delayed nausea and emesis in patients receiving moderately emetogenic chemotherapy: a phase III trial by the National Cancer Institute of Canada Clinical Trials Group. J ClinOncol 1994; 12:1050. 60.GrallaRJ, Navari RM, Hesketh PJ. Single-dose oral granisetron has equivalent antiemetic efficacy to intravenous ondansetron for highly emetogenic cisplatin-based chemotherapy. J ClinOncol 1998; 16:1568. 61.Keller GA, Ponte ML, Di Girolamo G. Other drugs acting on nervous system associated with QT-interval prolongation. Curr Drug Saf 2010; 5:105. 62.US Food and Drug Administration. Zofran (ondansetron): Drug Safety Communication - Risk of Abnormal Heart Rhythms. Available on: www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHum anMedicalProducts/ucm272041.htm 63.FDA
safety
communication
2010.
available
online
at
http://www.fda.gov/Drugs/DrugSafety/ucm237081.htm 64.Morganroth J, Flaharty KK, Parisi S, Moresino C. Effect of single doses of IV palonosetron, up to 2.25 mg, on the QTc interval duration: a double-blind, randomized, parallel group study in healthy volunteers. Support Care Cancer 2016; 24:621.
101
References 65.Likun Z, Xiang J, Yi B. A systematic review and meta-analysis of intravenous palonosetron in the prevention of chemotherapy-induced nausea and vomiting in adults. Oncologist 2011; 16:207. 66.Saito M, Aogi K, Sekine I. Palonosetron plus dexamethasone versus granisetron plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a double-blind, double-dummy, randomised, comparative phase III trial. Lancet Oncol 2009; 10:115. 67.Aapro MS, Grunberg SM, Manikhas GM, Olivares G, Suarez T, Tjulandin SA, et al. A phase III, double-blind, randomized trial of palonosetron compared with ondansetron in preventing chemotherapyinduced
nausea
and
vomiting
following
highly
emetogenic
chemotherapy. Ann Oncol 2006; 17:1441. 68.WHO Pharmaceuticals newsletter. Ondansetron and serotonin syndrome. 2012; 3:16. 69.dos Santos LV, Souza FH, Brunetto AT. Neurokinin-1 receptor antagonists for chemotherapy-induced nausea and vomiting: a systematic review. J Natl Cancer Inst 2012; 104:1280. 70.Campos D, Pereira JR, Reinhardt RR. Prevention of cisplatin-induced emesis by the oral neurokinin-1 antagonist, MK-869, in combination with granisetron and dexamethasone or with dexamethasone alone. J ClinOncol 2001; 19:1759. 71.Grunberg S, Chua D, Maru A. Single-dose fosaprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with cisplatin therapy: randomized, double-blind study protocol--EASE. J ClinOncol 2011; 29:1495. 72.McCrea JB, Majumdar AK, Goldberg MR. Effects of the neurokinin1 receptor antagonist aprepitant on the pharmacokinetics of dexamethasone and methylprednisolone. ClinPharmacolTher 2003; 74:17. 102
References 73.Warr DG, Hesketh PJ, Gralla RJ. Efficacy and tolerability of aprepitant for the prevention of chemotherapy-induced nausea and vomiting in patients with breast cancer after moderately emetogenic chemotherapy. J ClinOncol 2005; 23:2822. 74.Nygren P, Hande K, Petty KJ. Lack of effect of aprepitant on the pharmacokinetics
of
docetaxel
in
cancer
patients.
Cancer
ChemotherPharmacol 2005; 55:609. 75.Hesketh PJ, Rossi G, Rizzi G. Efficacy and safety of NEPA, an oral combination of netupitant and palonosetron, for prevention of chemotherapy-induced
nausea
and
vomiting
following
highly
emetogenic chemotherapy: a randomized dose-ranging pivotal study. Ann Oncol 2014; 25:1340. 76.Gralla RJ, Bosnjak SM, Hontsa A. A phase III study evaluating the safety and efficacy of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting over repeated cycles of chemotherapy. Ann Oncol 2014; 25:1333. 77.Schwartzberg LS, Modiano MR, Rapoport BL. Safety and efficacy of rolapitant for prevention of chemotherapy-induced nausea and vomiting after administration of moderately emetogenic chemotherapy or anthracycline and cyclophosphamide regimens in patients with cancer: a randomised, active-controlled, double-blind, phase 3 trial. Lancet Oncol 2015; 16:1071. 78.Rapoport BL, Chasen MR, Gridelli C. Safety and efficacy of rolapitant for prevention of chemotherapy-induced nausea and vomiting after administration of cisplatin-based highly emetogenic chemotherapy in patients with cancer: two randomised, active-controlled, double-blind, phase 3 trials. Lancet Oncol 2015; 16:1079. 103
References 79.Ioannidis JP, Hesketh PJ, Lau J. Contribution of dexamethasone to control of chemotherapy-induced nausea and vomiting: a meta-analysis of randomized evidence. J ClinOncol 2000; 18:3409. 80.Joss RA, Bacchi M, Buser K. Ondansetron plus dexamethasone is superior to ondansetron alone in the prevention of emesis in chemotherapy-naive and previously treated patients. Swiss Group for Clinical Cancer Research (SAKK). Ann Oncol 1994; 5:253. 81.Italian Group for Antiemetic Research. Double-blind, dose-finding study of four intravenous doses of dexamethasone in the prevention of cisplatin-induced acute emesis. J ClinOncol 1998; 16:2937. 82.Italian Group for Antiemetic Research. Randomized, double-blind, dosefinding study of dexamethasone in preventing acute emesis induced by anthracyclines, carboplatin, or cyclophosphamide:. J ClinOncol 2004; 22:725. 83.Todaro B. Cannabinoids in the treatment of chemotherapy-induced nausea and vomiting. J Natl ComprCancNetw 2012; 10:487. 84.Koo WH, Ang PT. Role of maintenance oral dexamethasone in prophylaxis of delayed emesis caused by moderately emetogenic chemotherapy. Ann Oncol 1996; 7:71. 85.The Italian Group for Antiemetic Research. Dexamethasone alone or in combination with ondansetron for the prevention of delayed nausea and vomiting induced by chemotherapy. N Engl J Med 2000; 342:1554. 86.Olver I, Paska W, Depierre A. A multicentre, double-blind study comparing placebo, ondansetron and ondansetron plus dexamethasone for the control of cisplatin-induced delayed emesis. Ondansetron Delayed Emesis Study Group. Ann Oncol 1996; 7:945.
104
References 87.Roila F, Ruggeri B, Ballatori E. Aprepitant versus dexamethasone for preventing chemotherapy-induced delayed emesis in patients with breast cancer: a randomized double-blind study. J ClinOncol 2014; 32:101. 88.Roila F, Ruggeri B, Ballatori E. Aprepitant versus metoclopramide, both combined with dexamethasone, for the prevention of cisplatin-induced delayed emesis: a randomized, double-blind study. Ann Oncol 2015; 26:1248. 89.Aapro M, Rugo H, Rossi G. A randomized phase III study evaluating the efficacy and safety of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy. Ann Oncol 2014; 25:1328. 90.Geling O, Eichler HG. Should 5-hydroxytryptamine-3 receptor antagonists be administered beyond 24 hours after chemotherapy to prevent delayed emesis? Systematic re-evaluation of clinical evidence and drug cost implications. J ClinOncol 2005; 23:1289. 91.Navari RM, Gray SE, Kerr AC. Olanzapine versus aprepitant for the prevention of chemotherapy-induced nausea and vomiting: a randomized phase III trial. J Support Oncol 2011; 9:188. 92.Tan L, Liu J, Liu X. Clinical research of Olanzapine for prevention of chemotherapy-induced nausea and vomiting. J ExpClin Cancer Res 2009; 28:131. 93.Roscoe JA, Heckler CE, Morrow GR. Prevention of delayed nausea: a University of Rochester Cancer Center Community Clinical Oncology Program study of patients receiving chemotherapy. J ClinOncol 2012; 30:3389.
105
References 94.Morrow GR, Roscoe JA, Kirshner JJ, Hynes HE, Rosenbluth RJ. Anticipatory nausea and vomiting in the era of 5-HT3 antiemetics. Support Care Cancer 1998; 6:244. 95.Roscoe JA, Bushunow P, Morrow GR. Patient expectation is a strong predictor of severe nausea after chemotherapy: a University of Rochester Community Clinical Oncology Program study of patients with breast carcinoma. Cancer 2004; 101:2701. 96.Fallowfield LJ. Behavioural interventions and psychological aspects of care during chemotherapy. Eur J Cancer 1992; 28A Suppl 1:S39. 97.Razavi D, Delvaux N, Farvacques C. Prevention of adjustment disorders and anticipatory nausea secondary to adjuvant chemotherapy: a doubleblind, placebo-controlled study assessing the usefulness of alprazolam. J ClinOncol 1993; 11:1384. 98.Räth U, Upadhyaya BK, Arechavala E. Role of ondansetron plus dexamethasone in fractionated chemotherapy. Oncology 1993; 50:168. 99.Albany C, Brames MJ, Fausel C. Randomized, double-blind, placebocontrolled, phase III cross-over study evaluating the oral neurokinin-1 antagonist aprepitant in combination with a 5HT3 receptor antagonist and dexamethasone in patients with germ cell tumors receiving 5-day cisplatin combination chemotherapy regimens: a hoosier oncology group study. J ClinOncol 2012; 30:3998. 100. Boccia RV, Gordan LN, Clark G. Efficacy and tolerability of transdermal granisetron for the control of chemotherapy-induced nausea and vomiting associated with moderately and highly emetogenic multiday chemotherapy: a randomized, double-blind, phase III study. Support Care Cancer 2011; 19:1609. 101. Mattiuzzi GN, Cortes JE, Blamble DA. Daily palonosetron is superior to ondansetron in the prevention of delayed chemotherapy-induced nausea 106
References and vomiting in patients with acute myelogenous leukemia. Cancer 2010; 116:5659. 102. Stiff P, Fox-Geiman M, Kiley K. Aprepitant vs. placebo plus oral ondansetron and dexamethasone for the prevention of nausea and vomiting associated with highly emetogenic preparative regimens prior to hematopoietic stem cell transplantation; A prospective, randomized double-blind phase III trial. Blood (ASH Annual Meeting Abstracts) 2009; 114:2267. 103. Yeh SP, Lo WC, Hsieh CY, Bai LY, Lin CC, Lin PH, et al. Palonosetron and dexamethasone for the prevention of nausea and vomiting in patients receiving allogeneic hematopoietic stem cell transplantation. Support Care Cancer 2014; 22:1199. 104. Stiff PJ, Fox-Geiman MP, Kiley K, Rychlik K, Parthasarathy M, Fletcher-Gonzalez D, et al. Prevention of nausea and vomiting associated with stem cell transplant: results of a prospective, randomized trial of aprepitant used with highly emetogenic preparative regimens. Biol Blood Marrow Transplant 2013; 19:49. 105. Schmitt T, Goldschmidt H, Neben K. Aprepitant, granisetron, and dexamethasone for prevention of chemotherapy-induced nausea and vomiting after high-dose melphalan in autologous transplantation for multiple myeloma: results of a randomized, placebo-controlled phase III trial. J ClinOncol 2014; 32:3413. 106. Navari RM, Nagy CK, Gray SE. The use of olanzapine versus metoclopramide for the treatment of breakthrough chemotherapyinduced nausea and vomiting in patients receiving highly emetogenic chemotherapy. Support Care Cancer 2013; 21:1655. 107. de Wit R, de Boer AC, vd Linden GH. Effective cross-over to granisetron after failure to ondansetron, a randomized double blind study 107
References in patients failing ondansetron plus dexamethasone during the first 24 hours following highly emetogenic chemotherapy. Br J Cancer 2001; 85:1099. 108. de Jong FA, Engels FK, Mathijssen RH. Medicinal cannabis in oncology practice: still a bridge too far? J ClinOncol 2005; 23:2886. 109. Vinciguerra V, Moore T, Brennan E. Inhalation marijuana as an antiemetic for cancer chemotherapy. N Y State J Med 1988; 88:525. 110. Bowles DW, O'Bryant CL, Camidge DR, Jimeno A. The intersection between cannabis and cancer in the United States. Crit Rev OncolHematol 2012; 83:1. 111. Russo EB, Guy GW, Robson PJ. Cannabis, pain, and sleep: lessons from therapeutic clinical trials of Sativex, a cannabis-based medicine. ChemBiodivers 2007; 4:1729. 112. Whiting PF, Wolff RF, Deshpande S. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA 2015; 313:2456. 113. Ryan JL, Heckler CE, Roscoe JA. Ginger (Zingiberofficinale) reduces acute chemotherapy-induced nausea: a URCC CCOP study of 576 patients. Support Care Cancer 2012; 20:1479. 114. Pillai AK, Sharma KK, Gupta YK, Bakhshi S. Anti-emetic effect of ginger powder versus placebo as an add-on therapy in children and young adults receiving high emetogenic chemotherapy. Pediatr Blood Cancer 2011; 56:234. 115. Panahi Y, Saadat A, Sahebkar A. Effect of ginger on acute and delayed chemotherapy-induced nausea and vomiting: a pilot, randomized, openlabel clinical trial. Integr Cancer Ther 2012; 11:204. 116. Zick SM, Ruffin MT, Lee J. Phase II trial of encapsulated ginger as a treatment for chemotherapy-induced nausea and vomiting. Support Care Cancer 2009; 17:563. 108
References 117. Fahimi F, Khodadad K, Amini S. Evaluating the effect of zingiberofficinalis on nausea and vomiting in patients receiving Cisplatin based regimens. Iran J Pharm Res 2011; 10:379. 118. Garcia MK, McQuade J, Haddad R. Systematic review of acupuncture in cancer care: a synthesis of the evidence. J ClinOncol 2013; 31:952. 119. Shen J, Wenger N, Glaspy J. Electroacupuncture for control of myeloablative chemotherapy-induced emesis: A randomized controlled trial. JAMA 2000; 284:2755. 120. Lotfi-Jam K, Carey M, Jefford M. Nonpharmacologic strategies for managing common chemotherapy adverse effects: a systematic review. J ClinOncol 2008; 26:5618. 121. Vidall C, Dielenseger P, Farrell C, Lennan E, Muxagata P, FernandezOrtega P, et al. Evidence-based management of chemotherapy-induced nausea and vomiting: a position statement from a European cancer nursing forum. Ecancermedicalscience 2011; 5:211. 122. Hesketh PJ, Kris MG, Grunberg SM. Proposal for classifying the acute emetogenicity of cancer chemotherapy. J ClinOncol 1999; 15:103-9. 123. Mohammed SS, Sheikha AK, Saaed AM, Sheet SY, Khasraw M. Histological types of non Hodgkin's lymphomas according to current WHO classifications in the Sulaymani province. J ClinOncol 2011; 29 (18550). 124. Hjalgrim D, Askling J, Pukkala E, Hansen S, Munksgaard L, Frisch M. Incidence of Hodgkin's disease in Nordic countries. The Lancet 2001; 358: 297-298. 125. Thomas RK, Re D, Zander T, Wolf J and Diehl V. Epidemiology and etiology of Hodgkin’s lymphoma. Ann Oncol 2002; 13 (4):147-152.
109
References 126. Mueller N, Grufferman S. Epidemiology. In Hodgkin's Disease, Mauch PM, Armitage J, Diehl V, Hopp R, Eiss LM (eds), Raven Press, Ltd.: New York 1999. 127. Yung L, Linch D. Hodgkin's lymphoma. Lancet 2003; 15; 361(9361): 943-951. 128. Hoffbrand AV, Catovsky D, Tuddenham EGD, Green AR. Postgraduate Hematology, Wiley-Blackwell, ISBN 978-4051-9180-7, Oxford2011. 129. Smith A, Crouch S, Lax S, Li J, Painter D, Howell D, et al. Lymphoma incidence, survival and prevalence 2004–2014: sub-type analyses from the UK’s Haematological Malignancy Research Network. British Journal of Cancer 2015; 112(9):1575-1584. 130. Shenoy P, Maggioncalda A, Malik N and Flowers CR. Incidence patterns and outcomes for Hodgkin’s lymphoma patients in the United States. Advances in Hematology 2011; 725219. 131. Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. Blood 2006; 107: 265–276. 132. Ng WL, Della-Fiorentina SA. The efficacy of oral ondansetron and dexamethasone for the prevention of acute chemotherapy-induced nausea and vomiting associated with moderately emetogenic chemotherapy - a retrospective audit. Eur J Cancer Care (Engl). 2010; 19(3):403-407. 133. Aziz F. Neurokinin-1 receptor antagonists for chemotherapy-induced nausea and vomiting. Ann Palliat Med 2012; 1(2):130-136. 134. Cocquyt V, Van Belle S, Reinhardt RR. Comparison of L-758,298, a prodrug for the selective neurokinin-1 antagonist, L-754,030, with ondansetron for the prevention of cisplatininduced emesis. Eur J Cancer. 2001; 37:835–842.
135. Navari
RM, Reinhardt RR, Gralla RJ. Reduction of cisplatin-induced emesis by a selective
neurokinin-1-receptor antagonist. L-754,030 Antiemetic Trials Group. N Engl J Med. 1999; 340:190–195.
110
References 136. Grote T, Hajdenberg J, Cartmell A, Ferguson S, Ginkil A, Charu V. Combination therapy for chemotherapy-induced nausea and vomiting in patients receiving moderately emetogenic chemotherapy: Palonosetron, dexamethasone, and aprepitant. J Support Oncol 2006; 4:403–408. 137. Chawla SP, Grunberg SM, Gralla RJ. Establishing the dose of the oral NK1 antagonist aprepitant for the prevention of chemotherapy-induced nausea and vomiting. Cancer 2003; 97:2290-300. 138. Schmoll HJ, Aapro MS, Poli-Bigelli S, Kim HK, Park K, Jordan K, et al. Comparison of an aprepitant regimen with a multiple-day ondansetron regimen, both with dexamethasone, for antiemetic efficacy in high-dose cisplatin treatment. Ann Oncol 2006; 17(6):1000-1006. 139. Poli-Bigelli S, Rodrigues-Pereira J, Carides AD, Julie Ma G, Eldridge K, Hipple A, et al. Addition of the neurokinin 1 receptor antagonist aprepitant to standard antiemetic therapy improves control of chemotherapy-induced nausea and vomiting. Results from a randomized, double-blind, placebo-controlled trial in Latin America. Cancer 2003; 97:3090-3098. 140. Grunberg
SM, Rolski J, Strausz J. Efficacy and
safety of
casopitantmesylate, a neurokinin 1 (NK1)-receptor antagonist, in prevention of chemotherapy-induced nausea and vomiting in patients receiving
cisplatin-based
highly
emetogenic
chemotherapy:
a
randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009; 10:549-558. 141. Hesketh PJ, Grunberg SM, Gralla RJ, Warr DG, Roila F, de Wit R, et al. The oral neurokinin-1 antagonist aprepitant for the prevention of chemotherapy-induced
nausea
and
vomiting:
a
multinational,
randomized, double-blind, placebo-controlled trial in patients receiving
111
References high-dose cisplatin--the Aprepitant Protocol 052 Study Group. J ClinOncol 2003; 21(22):4112-4119. 142. Cubeddu LX. Serotonin mechanisms in chemotherapy-induced emesis in cancer patients. Oncology 1996; 53 (1): 18–25. 143. Hesketh PJ, Van Belle S, Aapro M, Tattersall FD, Naylor RG, Hargreaves R, et al. Differential involvement of neurotransmitters through the time course of cisplatin-induced emesis as revealed by therapy with specific receptor antagonists. Eur J Cancer 2003; 39: 1074– 1080 144. Roila F, Donati D, Tamberi S, Margutti G. Delayed emesis: incidence, pattern, prognostic factors and optimal treatment. Support Care Cancer 2002; 10: 88–95. 145. Yeo W, Mo FK, Suen JJ, Ho WM, Chan SL, Lau W, et al. A randomized study of aprepitant, ondansetron and dexamethasone for chemotherapyinduced nausea and vomiting in Chinese breast cancer patients receiving moderately emetogenic chemotherapy. Breast Cancer Res Treat 2009; 113(3):529-535. 146. Hu W, Fang J, Nie J, Dai L, Chen X, Zhang J, et al. Addition of aprepitant improves
protection
conventional
against
anti-emetic
cisplatin-induced
regimen
Pharmacol 2014; 73(6):1129-1136.
112
fails.
emesis
Cancer
when
a
Chemother
Appendices
)Appendix (A هەرێمی کوردستانی عێراق
Iraqi Kurdistan Region Ministry of Higher Education and Scientific Research Faculty of Medical Sciences School of Pharmacy
وەزارەتی خوێندنی بااڵ و توێژینەوەی زانستی فاکەڵتی زانستە پزیشکییەکان سکوڵی دەرمانسازی
نەخۆشخانەی فێرکاری هیوا بۆ چارەسەری نەخۆشیەکانی شێرپەنجە و خوێن فۆرمی ڕازی بوون و بەشداری کردن لە توێژینەوەی زانستی بەروار /
من کە ناوم (
) بە بێ هەبوونی هیچ ف شارێک ڕەزامەندم بە بە شداری کردنم لەم توێژینەوەیەدا
لە ژێر چاااودێری یشیشاااااای دەرمااان ااااااااز (دارا عباادال اام م وااد) وە ڕەزامەناادم بە هەموو دەراەن ااامەکااانی
نەخۆش
یشیشای چارەسەر
Appendix (B) Nausea Domain 1. 2. 3. 4. 5. 6. 7. 8. 9.
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Quantity of nausea. Ability to maintain usual recreation or leisure activities. Ability to make a meal or do minor household repairs Ability to enjoy a meal. Ability to enjoy liquid refreshment. Willingness to spend time with family/friends. Affected daily functioning. Imposed personal hardship. Imposed hardship on others
Vomiting domain 1. 2. 3. 4. 5. 6. 7. 8. 9.
Quantity of vomiting Ability to maintain usual recreation or leisure activities. Ability to make a meal or do minor household repairs Ability to enjoy a meal. Ability to enjoy liquid refreshment. Willingness to spend time with family/friends. Affected daily functioning. Imposed personal hardship. Imposed hardship on others
)Appendix (C بواری ڕشانەوە 1 1. 2. 3. 4. 5. 6. 7. 8. 9.
2
3
4
5
6
7
8
9
10
توندیی ڕشانەوە توانستی کردنی چاالکی ئاسایی و چاالکیی کاتی بەتاڵ توانستی دروستکردنی چێشت یان کاری بچوکی ماڵ توانستی ئارەزوو کردن بە خواردنەوە توانستی ئارەزوو کردن بە خواردنەوەی فرێشەوە ئارەزووی بەسەر بردنی کات لەگەڵ خێزان و هاوڕێیان کاری ڕۆژانەی کارتێکراو فشار لەسەر سەختیی کەسی سەختی خستنە سەر کەسانی تر
بواری دڵ تێکهەاڵن
1 1. 2. 3. 4. 5. 6. 7. 8. 9.
توندیی دڵتێکهەاڵتن توانستی کردنی چاالکی ئاسایی و چاالکیی کاتی بەتاڵ توانستی دروستکردنی چێشت یان کاری بچوکی ماڵ توانستی ئارەزوو کردن بە خواردنەوە توانستی ئارەزوو کردن بە خواردنەوەی فرێشەوە ئارەزووی بەسەر بردنی کات لەگەڵ خێزان و هاوڕێیان کاری ڕۆژانەی کارتێکراو فشار لەسەر سەختیی کەسی سەختی خستنە سەر کەسانی تر
2
3
4
5
6
7
8
9
10
الخالصة مقدمة :الغثيان والقيء الناجم عن العالج الكيميائي سيكون دائما موجود طالما يتم استخدام العالجات الكيماوية المسببة لتسمم الخاليا في عالج السرطان .الغثيان والقيء من األعرا الشائعة و المخيفة بين مرضى السرطان ،و تصل نسبة حدوثها إلى ٪80من المرضى الذين يستخدمون العالج الكيميائي دون عالج وقائي. الهدف من الدراسة :لمقارنة تأثير مضاد القىء الحاد و المتأخر االمد والتغيير في نوعية الحياة لالدوية (ابريبيتانت ،أوندانسيترون وديكساميثازون) واالدوية (أوندانسيترون و ديكساميثازون) في المرضى الذين يتلقون العالج الكيميائي المسبب للغثيان والقئ في مستشفى هيوا التعليمي المرا
السرطان في السليمانية /اقليم كردستان .
المرضى وطرق البحث :تجربة سريرية منضبطة ذات االتجاه الواحد أجريت في مستشفى هيوا التعليمي للسرطان في مدينة السليمانية للفترة من 1يناير إلى نهاية ديسمبر 2015 ،على عينة مناسبة من 70مريض مصاب بداء هودجكين .وتلقى المرضى إما العالج (ابريبيتانت، أوندانسيترون وديكساميثازون) أو نظام العالج القياسي (أوندانسيترون و ديكساميثازون) بنسبة 1 :1وفقا لذلك ،وحسب جدول التخصيص العشوائي الحاسوبي. النتائج :لم يكن هناك فرق كبير بين مجموعتين الدراسة في متوسط درجات الغثيان في اليوم األول ( .)p=0.3ولوحظ وجود عالقة ذو داللة احصائية بين ارتفاع متوسط عالمات التأثير المضاد للغثيان والقئ ومرضى مجموعة العالج في االيام الثانية والثالثة من العالج بالمقارنة مع مرضى المجموعة القياسية ( .)<0.05بشكل عام كان هناك ارتفاع متوسط عالمات التأثير المضاد للغثيان والقئ بين مرضى مجموعة العالج بالمقارنة مع مرضى المجموعة القياسية ).(p=0.001 االستنتاجات :استخدام أدوية ابريبيتانت ،أوندانسيترون وديكساميثازون أظهر نتائج متفوقة وذات قيمة في الوقاية من الغثيان والقيء الناجم عن العالج الكيميائي لمرضى السرطان.
جمهورية العراق اقليم كوردستان وزارة التعليم العالي والبحث العلمي جامعة السليمانية كلية الصيدلة
مقارنة لتأثيرمضاد القىء الحاد و المتأخر االمد والتغييرفي نمط الحياة لالدوية (ابريبيتانت،أوندانسيترون وديكساميثازون) واالدوية (أوندانسيترون وديكساميثازون) في المرضى الذين يتلقون العالج الكيميائي المسبب للغثيان والقئ في مستشفى هيوا المراض السرطان في السليمانية قدمت هذه الدراسة الى مجلس كلية الصيدلة /جامعة السليمانية كاحدى متطلبات الحصول على شهادة الماجستير في اختصاص الصيدلة السريرية
دارا عبدهللا محمد بكالوريوس في الصيدلة 2012 - 2011 المشرف
د.مي الصباغ بروفيسورة المساعدة /كلية الصيدلة -جامعة بغداد
2016ميالدي
1438هجري
2716كوردي
پوختە پێشەکی دڵ تێکهەڵهاتن و ڕشانەوەی دروست بوو بەهۆی وەرگرتنی دەرمانی کیمیاوی شێرپەنجە بەردەوام دەبێت بە درێژایی بەردەوام بوونی وەرگرتنی دەرمانەکان ،دڵ تێکهەڵهاتن و ڕشاااااااانەوە ۆرترین و ترساااااااناکترین کاریگەری الوەکی دەرمانی کیمیاویەکانن ،بە ڕێژەیەک کە %٨٠نەخۆشااەکان توشاای دەبن رەگەر دەرمانی خۆپاراستنی بۆ بەکار نەهێنن . ئامانجی توێژینەوەکە بەراورد کردنی کاریگەری ساااااەرەتایی و درێژخایەنی دڵ تێکهەڵهاتن و ڕشاااااانەوە هەروەها گۆڕانکاری لە جۆری ژیانی رەو نەخۆشااانەی کە (رەپریپیتانت ،رۆندانساایترۆن ،دێکسااامیسااا ۆن بەکار دەهێنن لەگەڵ رەو نەخۆشااانەی (رۆندانساایترۆن ،دێکسااامیسااا ۆن بەکاردەهێنن لەکاتی وەرگرتنی رەو دەرمانە کیمیاویانەی کە دەبنە هۆی دروساااتبونی دڵ تێکهەڵهاتن و ڕشاااانەوەی ۆر لە نەخۆشاااخانەی فێرکاری هیوا بۆ چارەساااەری نەخۆشیەکانی شێرپەنجە لە شاری سلێمانی . نەخۆشی و ڕێگاکانی لێکۆڵینەوە توێژینەوەیەکی تاک راراستەی کۆنترۆڵ کراو لە نەخۆشخانەی هیوا لە شاری سلێمانی لە ماوەی 2015/1/1 هەتاکو 2015/12/1لەساااااااەر 70نەخۆشااااااای ( هۆجکن لیم ۆما کە نەخۆشاااااااەکان یاخود (رەپریپیتانت ، رۆندانسااایترۆن ،دێکساااامیساااا ۆن یان (رۆندانسااایترۆن ،دێکساااامیساااا ۆن وەردەگرن بە ڕێژەی ( 1:1کە پرۆگرامێکی کۆمپیوتەری بە پێی ڕاندۆم رەلۆکەیشن دیاری دەکات . ئەنجام هیچ جیاوا ییەکی کاریگەر نەبوو لە نێوان هەردوو جۆری دەرمانەکان لە ڕێژەی دڵ تێکهەڵهاتن لە ڕۆژی یەکەمی چااارەساااااااەر کردن ( . P=0.3جیاااوا ییەکی بەرچاااو هەبوو لەو نەخۆشاااااااااانەی (رەپریپیتاااناات ، رۆندانسااااایترۆن ،دێکساااااامیساااااا ۆن یان وەرگرت لە هەردوو بواری دڵ تێکهەڵهاتن و ڕشاااااانەوە لە ڕۆژی دووهەم و سااااااا هەم و چوارەم ( P=0.05بە بەراورد بەو نەخۆشااااااااانەی کە تەنهااا (رۆناادانسااااااایترۆن ، دێکسامیسا ۆن یان وەرگرتووە . دەرئەنجام بەکارهێنانی (رەپریپیتانت ،رۆندان سیترۆن ،دێک سامی سا ۆن رەنجامی بەر تر و با شتری نی شاندا لە ڕێگرتن بە توشاابوونی ،دڵ تێکهەڵهاتن و ڕشااانەوە لەو نەخۆشااانەی دەرمانی کیمیاوی بەکار دەهێنن بۆ چارەسااەری نەخۆشی شێرپەنجە .
کۆماری عێراق هەرێمی کوردستان وەزارەتی خوێندنی بااڵ و توێژینەوەی زانستی زانکۆی سلێمانی کۆلێژی دەرمانسازی
بەراورد کردنی کاریگەری دژە دڵتێکچونی سەرەتایی و درێژخایەن و گۆڕانکاری لە جۆری ژیانی ئەو نەخۆشانەی کە (ئەپریپیتانت ،ئۆندانسیترۆن ،دێکسامیسازۆن) و (ئۆندانسیترۆن ،دێکسامیسازۆن) بەکاردەهێنن لەکاتی وەرگرتنی ئەو دەرمانە کیمیاویانەی کە دەبنە هۆی دروستبونی دڵ تێکچوون و ڕشانەوەی زۆر لە نەخۆشخانەی هیوا بۆ چارەسەری نەخۆشیەکانی شێرپەنجە . نامەیەکە پێشکەش کراوە بە ئەنجومەنی کۆلێژی دەرمانسازی لە زانکۆی سلێمانی وەکو بەشێک لە پێداویستیەکانی بەدەستهێنانی بڕوانامەی ماستەر لە بواری دەرمانسازی کلینیکی
دارا عبدهللا محمد بەکالۆریۆس لە دەرمانسازیدا 2012 - 2011 بەسەرپەرشتی
د .مي الصباغ پڕۆفیسۆری یاریدەدەر /کۆلێژی دەرمانسازی /زانکۆی بەغداد
2016زایینی
1438کۆچی
2716کوردی