Respirology (2007) 12, 670–674
doi: 10.1111/j.1440-1843.2007.01114.x
ORIGINAL ARTICLE
Changes in circulating thrombomodulin levels with exercise in patients with chronic obstructive pulmonary disease Hiroshi KANAZAWA, Kazuhisa ASAI AND Saeko NOMURA Department of Respiratory Medicine, Graduate School of Medicine, Osaka City University, Osaka, Japan
Changes in circulating thrombomodulin levels with exercise in patients with chronic obstructive pulmonary disease KANAZAWA H, ASAI K, NOMURA S. Respirology 2007; 12: 670–674 Background and objectives: The functional properties of endothelial cells in pulmonary microvessels are affected by elevations in the level of vascular endothelial growth factor (VEGF) in inflamed airways. An increase in the level of circulating thrombomodulin (TM), a molecular marker of endothelial cells, with exercise is associated with the VEGF level in asthmatic airways. This study investigated whether the airway VEGF level reflects changes in circulating TM levels with exercise in patients with COPD. Methods: VEGF levels in induced sputum were measured in 26 COPD patients (12 chronic bronchitis and 14 emphysema) and 11 control subjects. Incremental exercise testing was performed, and TM levels in arterial blood samples were measured pre-exercise and post-exercise at 0, 5 and 60 min. Results: VEGF levels were significantly lower in patients with emphysema (520 ⫾ 290 pg/mL) than in control subjects (1860 ⫾ 1220 pg/mL), and were significantly higher in patients with bronchitis (4110 ⫾ 1190 pg/mL). Pre-exercise TM levels were comparable among the three study groups. TM levels in control subjects and emphysema patients did not change after exercise. However, maximum TM levels after exercise were significantly increased in chronic bronchitis patients (P = 0.02). The increase in TM level with exercise closely correlated with the VEGF level in bronchitis patients (r = 0.90, P = 0.003). Conclusions: In chronic bronchitis, but not in emphysema, patients exercise induced an increase in circulating TM levels. The potential causal relationship between circulating levels of TM and those of VEGF in the airways deserve further exploration. Key words: exercise, induced sputum, pulmonary endothelial cell, thrombomodulin, vascular endothelial growth factor.
INTRODUCTION COPD, a syndrome of variable phenotype, is mostly caused by inhaled cigarette smoke. Over time, alveolar destruction results in emphysema, and chronic airway inflammation leads to chronic bronchitis. In chronic bronchitis, airway inflammation is associated with structural alterations including an increase in the amount of smooth muscle and connective tissue Correspondence: Hiroshi Kanazawa, Department of Respiratory Medicine, Graduate School of Medicine, Osaka City University, 1-4-3, Asahi-machi, Abenoku, Osaka 545-8585, Japan. Email: kanazawa-h@med. osaka-cu.ac.jp Received 9 August 2006; invited to revise 11 December 2006; revised 25 December 2006; accepted 23 January 2007 (Associate Editor: Toshihiro Nukiwa).
in the airway wall.1 Airway microvessel proliferation has been shown to be a feature of inflammatory airway diseases,2 suggesting that active airway inflammation might also affect microvascular remodelling in chronic bronchitis. In contrast, it has been hypothesized that emphysema may lead to loss of pulmonary microvessels.3 Little is known about the molecular mechanisms underlying these processes in different phenotypes of COPD and it is not certain which mediators are involved in the mechanisms of airway microvascular remodelling. Several studies have indicated that one of the most potent mediators involved in this process is vascular endothelial growth factor (VEGF).4 VEGF promotes an array of responses, including in endothelial cell proliferation and angiogenesis with new vessel formation in vivo. 5 Previous studies have reported that VEGF expression was increased in asthmatic airways, and that its levels were closely correlated with airway vascularity.6
© 2007 The Authors Journal compilation © 2007 Asian Pacific Society of Respirology
671
Soluble thrombomodulin in COPD
However, airway microvascular remodelling may result not only in more and larger blood vessels in the mucosa, but also in functionally abnormal blood vessels, which exhibit sustained leakage. These findings indicate that the functional properties of pulmonary endothelial cells may be affected by elevated VEGF level in inflamed airways. Thrombomodulin (TM) is a component of the plasma membrane of vascular endothelial cells, and elevated levels of circulating TM reliably reflect progressive endothelial cell injury.7 Circulating TM levels in asthmatic patients are significantly increased after exercise, and this increase in the level of TM with exercise is associated with the VEGF level in the airways.8 It is our hypothesis that the change in plasma TM level with exercise may be a marker of the functional properties in VEGF-stimulated endothelial cells in human subjects. This study investigated whether airway VEGF level reflects change in TM level with exercise in patients with COPD.
each of two successive years; other causes of chronic cough were excluded. Emphysema was defined as abnormal permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls. Thus, bronchitis was defined in clinical terms, and emphysema in terms of anatomic pathology, based on the results of highresolution CT scans of the lungs. All patients with emphysema had low attenuation areas, whereas none of the patients with bronchitis did. Patients with COPD were treated with an inhaled anticholinergic drug, but none received oral or inhaled corticosteroids. Medications for the patients with COPD were not changed during the 1-month period preceding the study and were withdrawn at least 12 h before spirometric study, sputum induction, and exercise testing. No subjects in this study had been subjects in previous studies, and there was thus no overlap in the data of this study. All subjects gave written informed consent for participation in the study, which was approved by the ethics committee of Osaka City University.
METHODS Subjects
Exercise challenge testing
Twenty-six patients with COPD and 11 age-matched control subjects (all male) were included in this study. All control subjects were healthy, ex-smokers who had no history of lung disease. Patients with COPD, who had a history of previous smoking (>20 pack-years), were randomly selected from the respiratory outpatient clinic of the study institution and all satisfied the Global Initiative for Chronic Obstructive Lung Disease criteria.9 All patients were non-atopic (i.e. they had negative skin tests for common allergen extracts) and had no history of asthma or allergic rhinitis. Each subject underwent an interview, CXR, routine blood tests and skin tests with common allergen extracts. Pulmonary function tests were performed in the week preceding this study. DLCO was measured by the single-breath carbon monoxide method at least twice. The 10-second breath holding time was uniform in each subject. Since all COPD patients had a baseline FEV1 < 80% predicted, FEV1 measurement was repeated 15 min after the inhalation of 200 mg of salbutamol in order to assess the reversibility of airway obstruction. None of the patients exhibited reversibility of airway obstruction. Before exercise challenge testing, all COPD patients had right heart catheterization to estimate their pulmonary arterial pressure (PAP). All patients were clinically stable, and free of respiratory infection for at least 4 weeks before the study. No COPD patient had experienced an exacerbation of their disease, defined as increased dyspnoea associated with a change in the quality and quantity of sputum that led the subject to seek medical attention, during the 1-month period preceding the study. Clinical types of COPD were classified according to the criteria of the American Thoracic Society;10 14 patients had emphysema and 12 had chronic bronchitis. Chronic bronchitis was defined as the presence of cough and sputum production for 3 months in
Exercise testing was performed on a treadmill with continuous ECG monitoring. The general guidelines for exercise testing were followed.11 The patients exercised on a treadmill following a continuous multistage schedule with a 3-min duration of each stage. In COPD patients, initial workload was started at the speed of 0.75 mile per hour (mph) and no incline, followed by increments of 0.25 mph and 2–4% gradient at each stage. This progressive incremental exercise testing was performed until a symptom-limited maximum was reached. Arterial blood gas tensions (PaO2) were measured with a blood gas analyser (Model IL1312; Instrumentation Laboratory).
Sputum induction and processing Sputum induction was performed 3 days after the exercise challenge test, as previously described.12 The sputum sample diluted with PBS containing dithiothreitol (a final concentration of 1 mM) was then centrifuged at 400 g for 10 min. The supernatant was stored at -70°C for subsequent assay of VEGF. VEGF concentration was measured with an enzyme-linked immunosorbent assay (ELISA) kit (R&D system Inc, Minneapolis, MN, USA). The minimum detectable level of VEGF in this assay system is 5.0 pg/mL. All subjects produced an adequate specimen of sputum; a sample was considered adequate if the patient was able to expectorate at least 2 mL of sputum.
Measurements of TM Blood samples were obtained from arterial catheters, and collected in tubes containing citrate anticoagulant (1:9 in 3.8% citrate) for measurement of the TM level. All samples were kept at 4°C, centrifuged (2500 g
© 2007 The Authors Journal compilation © 2007 Asian Pacific Society of Respirology
672
H Kanazawa et al.
for 15 min at 4°C) within 30 min of collection, and stored at -80°C until the time of assay. Commercial ELISA kits were used for measurement of plasma TM (Diagnostica Stago, Paris, France). Plasma TM levels were measured at pre-exercise and post-exercise 0, 5 and 60 min.
levels were comparable in the three groups (controls: 3.4 ⫾ 1.0 ng/mL; emphysema patients: 3.4 ⫾ 0.8 ng/ mL; chronic bronchitis patients: 3.3 ⫾ 1.0 ng/mL) (Fig. 2). TM levels in control subjects or emphysema patients did not change pre- to post-exercise (postexercise maximum TM: controls: 3.4 ⫾ 0.9 ng/mL; emphysema patients: 3.4 ⫾ 0.9 ng/mL). However, post-exercise TM levels were significantly increased in chronic bronchitis patients (4.3 ⫾ 1.2 ng/mL, P = 0.02). Moreover, the increase in circulating TM levels with exercise (DTM = TM (post-exercise level)—TM (pre-exercise level)) closely correlated with VEGF level in induced sputum from chronic bronchitis patients (r = 0.90, P = 0.003) (Fig. 3).
Statistical analysis All values are presented as mean ⫾ SD. Multiple comparisons among groups were analysed by one-way analysis of variance by the Bonferroni’s correction. The significance of correlations was evaluated by determining Spearman rank correlation coefficients. A P-value of less than 0.05 was considered significant.
DISCUSSION RESULTS
7000 VEGF in sputum (pg/mL)
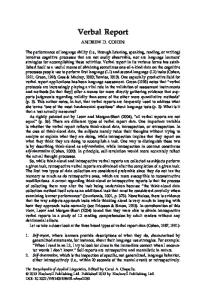
The clinical characteristics of the 26 COPD patients (12 bronchitis patients and 14 emphysema patients) and 11 control subjects are summarized in Table 1. The three groups were well matched with respect to age and smoking index. However, baseline pulmonary function values were significantly lower in patients with bronchitis or emphysema than in control subjects, and DLCO was also decreased in COPD patients. No COPD patient had severe pulmonary hypertension, and the maximum workload was comparable in the bronchitis and emphysema groups (stage III/ IV/V/VI, bronchitis group: 3/2/5/2; emphysema group: 3/3/6/2). PaO2 values were comparable in these two groups (bronchitis group: pre-exercise 73 ⫾ 6 mm Hg, post-exercise 63 ⫾ 7 mm Hg; emphysema group: pre-exercise 70 ⫾ 6 mm Hg, postexercise 61 ⫾ 7 mm Hg). VEGF levels in induced sputum were significantly lower in patients with emphysema (520 ⫾ 290 pg/mL, P = 0.002) than in control subjects (1860 ⫾ 1220 pg/mL) and significantly higher in patients with bronchitis (4110 ⫾ 1190 pg/mL, P < 0.0001) (Fig. 1). Serial measurement of soluble TM levels in plasma was performed in each COPD patients pre-exercise and post-exercise at 0, 5 and 60 min. Pre-exercise TM
This study found no significant differences in preexercise TM levels between control subjects, emphysema patients and chronic bronchitis patients.
*
6000 5000 4000 3000 2000
*
1000 0 Control subjects
Emphysema type
Bronchitis type
COPD patients
Figure 1 Comparison of vascular endothelial growth factor (VEGF) levels in induced sputum in control subjects, emphysema patients and bronchitis patients. *P < 0.01 compared with control subjects.
Table 1 Clinical characteristics of study subjects COPD patients
Number of subjects Age (years) FEV1 (% predicted) FEV1/FVC (% predicted) DLCO (%) Smoking index (pack-years) mPAP (mm Hg)
Control subjects
Bronchitis type
Emphysema type
11 61 (3.0) 80.2 (4.2) 71.0 (3.3) ND 29.9 (5.8) ND
12 63 (4.6) 52.3 (13.7)* 46.4 (8.6)* 48.9 (9.8) 33.9 (7.3) 24.3 (2.1)
14 62 (5.6) 48.9 (13.2)* 42.4 (7.8)* 38.9 (7.3) 33.4 (6.9) 23.8 (3.3)
*P < 0.01 compared with control subjects. All values are mean (SD). mPAP, mean pulmonary arterial pressure; ND, not determined.
© 2007 The Authors Journal compilation © 2007 Asian Pacific Society of Respirology
673
Soluble thrombomodulin in COPD
*
6.5 6
TM (ng/mL)
5.5 5 4.5 4 3.5 3 2.5 2 1.5 Pre
Post
Control subjects
Pre
Post
Emphysema type
Pre
Post
Bronchitis type
COPD patients
Figure 2 Comparison of plasma concentrations of soluble thrombomodulin (TM) pre-exercise (pre) and post-exercise 0 min (post) in control subjects, emphysema patients and bronchitis patients. *P < 0.05 compared with pre-exercise.
1.6
r = 0.90 P = 0.003
D TM (ng/mL)
1.4 1.2 1 0.8 0.6 0.4 0.2 2500
3500
4500
5500
6500
VEGF (pg/mL)
Figure 3 Correlation between vascular endothelial growth factor (VEGF) levels in induced sputum and the increase in soluble thrombomodulin (TM) levels in plasma with exercise (DTM: TM levels post-exercise 0 min—TM levels pre-exercise) in bronchitis patients.
Previous reports on resting TM levels in COPD patients have been conflicting. Plasma TM levels have been reported to be significantly decreased in COPD patients compared with control subjects.13 and also to be significantly increased in COPD patients without severe pulmonary hypertension compared with control subjects.14 This apparent discrepancy may be due to the different populations examined among the studies. It has also been reported that plasma TM levels are inversely correlated with the level of PAP.15 The COPD patients in the present study did not have severe pulmonary hypertension, which may explain the absence of decreased levels of plasma TM before exercise in COPD patients. Other possible explanations for the different findings are the use of venous blood for the measurement of plasma TM levels (in
the previous studies) rather than arterial blood (as was used in the present study), and drug effects, as COPD patients in the previous studies were taking a variety of drugs including steroids, angiotensinconverting enzyme inhibitors, and antiplatelet drugs, whereas COPD patients in the present study were not taking drugs that could affect the plasma TM level. A previous study reported that the highest level of TM was found in lung.16 Ebina et al. compared the pulmonary capillary endothelial cells according to their immunoreactivity for CD34, von Willebrand factor (vWf), and TM because of the phenotypic heterogeneity of pulmonary vascular endothelial cells.17 They confirmed that pulmonary capillary endothelial cells were intensely immunoreactive with CD34 and TM, but rarely with vWf. Investigation of plasma vWf levels as preliminary work for the present study showed they did not significantly change after postexercise in the three groups. More recently, Feltis et al. found that vWf is not present on VEGF-stimulated pulmonary endothelial cells.18 These findings suggest that TM is preferentially expressed in pulmonary microvessels,19 and is therefore considered to be a selective marker of pulmonary microvascular endothelium.20,21 The concentration of TM from the pulmonary microcirculation is significantly diluted when the blood reaches to the systemic circulation. This makes it detection of significant differences in TM levels difficult in humans. Despite this, a significant increase in the level of circulating TM with exercise was found in patients with chronic bronchitis. Therefore, increase in circulating TM level with exercise may be a sensitive marker of the functional properties of pulmonary endothelial cells of chronic bronchitis patients. The physiological and pathological significance of circulating TM is not unknown. It has been reported that circulating TM is very low compared with cellular TM in physiological activity. It is also possible that an increase in the circulating TM levels with exercise may lead to a decrease in TM expression on the endothelial cells. TM is the endothelial surface site for binding and inactivating thrombin, suggesting that TM is powerful inhibitor of thrombin. Thrombin has a potent mitogenic activity for various lung cells, and may be the mediator stimulating airway remodelling.22 Therefore, a decrease in TM on the pulmonary endothelial cell surface after exercise may induce the antithrombin activity of endothelium, leading to thrombin-mediated airway remodeling. Plasma TM levels in control subjects and emphysema patients did not change pre- to post-exercise. A previous study reported that plasma TM levels are stable in physiological conditions, and that fluctuation of the TM level is very slight.23 It thus appears that plasma TM levels in control subjects and emphysema patients may not be sensitive to exercise challenge. In contrast, post-exercise TM levels were significantly higher than pre-exercise levels in bronchitis patients, and the increase in soluble TM levels with exercise correlated with the VEGF level in bronchitis patients. Pulmonary endothelial cells stimulated by elevated levels of VEGF are sensitive to exercise challenge in patients with chronic bronchitis. Until now, a direct and non-invasive assessment of pulmonary
© 2007 The Authors Journal compilation © 2007 Asian Pacific Society of Respirology
674 endothelial cell injury in humans has not been possible in clinical practice. Even with use of an invasive method, only one lung segment and only one small tissue sample per patient has been available for examination and the information derived from such samples may not be representative of the entire lung. Measurement of the circulating TM level might reflect the injury in pulmonary endothelial cells of the entire lung in bronchitis patients. Though exercise-induced hypoxaemia leads to pulmonary endothelial cell dysfunction, there were no significant differences in PaO2 after exercise between emphysema and bronchitis patients. This disproves the hypothesis that exerciseinduced hypoxaemia leads to the increase in circulating TM levels in patients with bronchitis. In summary, this study found elevated levels of VEGF in induced sputum and raised circulating levels of TM in patients with chronic bronchitis. Future studies are needed to explore the potential biological links between these two observations, including morphological analysis of pulmonary microvessels, in chronic bronchitis patients.
ACKNOWLEDGEMENTS We thank Miss Yukari Matsuyama (Osaka City University, Osaka, Japan) for her help in the preparation and editing of the manuscript. This work was supported by a Grant-in-Aid for Scientific Research (No. 17590800) from the Japan Society for the Promotion of Science.
REFERENCES 1 Rennard SI. Inflammation and repair processes in chronic obstructive lung disease. Am. J. Respir. Crit. Care Med. 1999; 160: S12–16. 2 McDonald DM. Angiogenesis and remodeling of airway vasculature in chronic inflammation. Am. J. Respir. Crit. Care Med. 2001; 164: S39–45. 3 Kasahara Y, Tuder RM, Taraseviciene-Stewart L, Le Cras TD, Abman S et al. Inhibition of VEGF receptors causes lung cell apoptosis and emphysema. J. Clin. Invest. 2000; 106: 1311–19. 4 Kranenburg AR, de Boer WI, Alagappan VKT, Sterk PJ, Sharma HS. Enhanced bronchial expression of vascular endothelial growth factor and receptors (Flk-1 and Flt-1) in patients with chronic obstructive pulmonary disease. Thorax 2005; 60: 106–13. 5 Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr. Rev. 1997; 18: 4–25. 6 Hoshino M, Takahashi M, Aoike N. Expression of vascular endothelial growth factor, basic fibroblast growth factor, and angiogenin immunoreactivity in asthmatic airways and its relationship to angiogenesis. J. Allergy Clin. Immunol. 2001; 107: 295–301. 7 Iwashima Y, Sato T, Watanabe K, Ooshima E, Hiraishi S et al. Elevation of plasma thrombomodulin level in diabetic patients with early diabetic nephropathy. Diabetes 1990; 39: 983–8.
H Kanazawa et al. 8 Kanazawa H, Tochino Y, Ichimaru Y, Kodama T, Kyoh S et al. Role of vascular endothelial growth factor in pulmonary endothelial cell injury by exercise challenge in asthmatic patients. J. Asthma 2006; 43: 267–71. 9 Global Initiative for Chronic Obstructive Lung disease. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease. NHLBI/WHO Workshop Report. National Heart, Lung, and Blood Institute, Bethesda, 2001. Update of the management sections 2003. 10 American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease (COPD) and asthma. Am. Rev. Respir. Dis. 1987; 136: 225–44. 11 Kurihara N, Fujimoto S, Terakawa K, Yamamoto M, Takeda T. Prediction of PaO2 during treadmill walking in patients with COPD. Chest 1987; 91: 328–32. 12 Kanazawa H, Nomura S, Yoshikawa J. Role of microvascular permeability on physiologic differences in asthma and eosinophilic bronchitis. Am. J. Respir. Crit. Care Med. 2004; 169: 1125–30. 13 Cella G, Sbarai A, Mazzaro G, Vanzo B, Romano S et al. Plasma markers of endothelial dysfunction in chronic pulmonary disease. Clin. Appl. Thromb. Hemost. 2001; 7: 205–8. 14 Cella G, Saetta M, Baraldo S, Turato G, Papi A et al. Endothelial cell activity in chronic obstructive pulmonary disease without severe pulmonary hypertension. Clin. Appl. Thromb. Hemost. 2005; 11: 435–40. 15 Cella G, Bellotto F, Tona F, Sbarai A, Mazzaro G et al. Plasma markers of endothelial dysfunction in pulmonary hypertension. Chest 2001; 120: 1226–30. 16 Ishii H, Salem H, Bell CE, Laposata EA, Majerus PW. Thrombomodulin, an endothelial anticoagulant protein, is absent from the human brain. Blood 1986; 67: 362–5. 17 Ebina M, Shimizukawa M, Shibata N, Kimura Y, Suzuki T et al. Heterogeneous increase of CD34-positive alveolar capillaries in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2004; 169: 1203–8. 18 Feltis BN, Wignarajah D, Zheng L, Ward C, Reid D et al. Increased vascular endothelial growth factor and receptors. Relationship to angiogenesis in asthma. Am. J. Respir. Crit. Care Med. 2006; 173: 1201–7. 19 Frijns R, Fijnheer R, Schiel A, Donders R, Sixma J et al. Persistent increase in plasma thrombomodulin in patients with a history of lupus nephritis: endothelial cell activation markers. J. Rheumatol. 2001; 28: 514–19. 20 Ford VA, Stringer C, Kennel SJ. Thrombomodulin is preferentially expressed in Balb/c lung microvessels. J. Biol. Chem. 1992; 267: 5446–50. 21 Yamamoto M, Shimokata K, Nagura H. An immunohistochemical study on phenotypic heterogeneity of human pulmonary vascular endothelial cells. Virchows Arch. A 1988; 412: 479–86. 22 Reed CE, Kita H. The role of protease activation of inflammation in allergic: respiratory diseases. J. Allergy Clin. Immunol. 2004; 114: 997–1008. 23 Ishii H, Nakano M, Tsubouchi J, Ishikawa T, Uchiyama H et al. Establishment of enzyme immunoassay of human thrombomodulin in plasma and urine using monoclonal antibodies. Thromb. Haemost. 1990; 63: 157–62.
© 2007 The Authors Journal compilation © 2007 Asian Pacific Society of Respirology